





















Prospective or Concurrent RAF Capture: The Real Question Is Physician Burden
Most organizations frame the prospective versus concurrent RAF capture decision as a coding question. It is not. At the CMO level, it is a physician burden question, one that determines how much documentation load you place on your clinical workforce, where your HCC gaps will appear, and whether your risk adjustment program is sustainable at scale. The capture model you choose determines how often physicians disengage from documentation workflows, and disengagement is where RAF accuracy goes to die.
Both approaches can improve RAF accuracy. But they do it through different mechanisms, at different points in the care cycle, and with different implications for your physicians. Choosing between them without accounting for that difference is where most RAF programs quietly lose ground. The shift to the V28 risk adjustment model has added another variable: which conditions are captured at all, and how documentation specificity is rewarded, have changed in ways that make capture strategy decisions more consequential than they were under prior model versions.
What Is the Actual Difference Between Prospective and Concurrent RAF Capture?
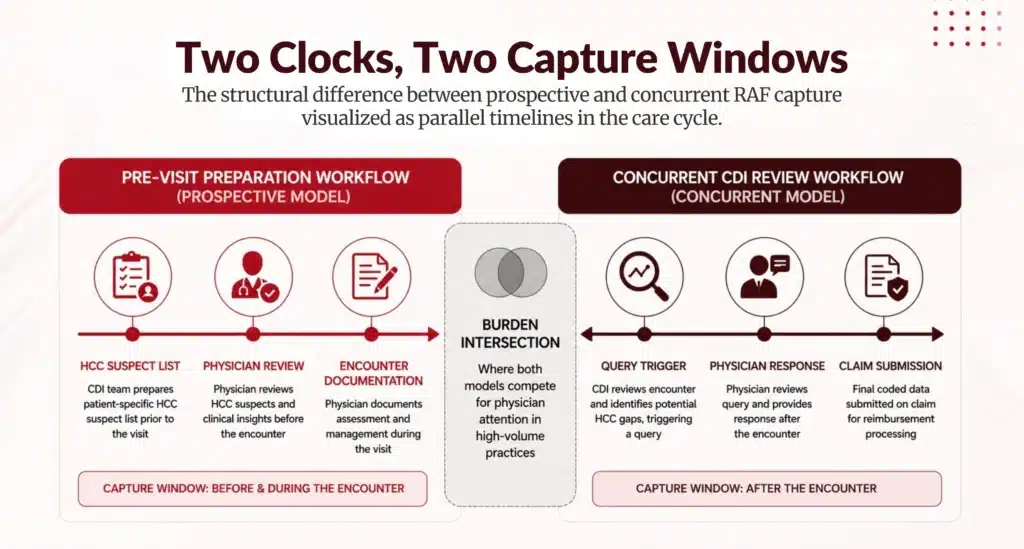
Prospective RAF capture targets documentation gaps before the patient encounter. Using prior claims data, care gap reports, and predictive analytics, clinical teams prepare physicians with a suspect HCC list ahead of the visit. The physician addresses those conditions during the encounter if clinically appropriate, and the documentation reflects it. The capture opportunity lives in pre-visit preparation.
Concurrent RAF capture works differently. A CDI specialist or coder reviews the in-progress encounter, typically within 24 to 48 hours, and flags underdocumented conditions, and submits a physician query before the claim closes. The physician responds, documentation improves, and the claim goes out at the correct specificity. The capture opportunity lives in real-time clinical review.
Both models move HCC accuracy. What they move differently is where physician attention is required and when. Prospective capture asks physicians to act before the visit. Concurrent capture asks them to respond after it. Neither is passive, and neither is zero-burden, which is precisely why the CMO framing matters.
Where Each Model Places Burden on Physicians
Prospective Capture and the Pre-Visit Documentation Load
Prospective RAF programs depend on physician compliance with pre-visit workflows. If your EHR surfaces a suspect HCC list that physicians are expected to review before each encounter, you are adding a structured cognitive task to an already compressed visit schedule. For organizations with high panel volumes, this burden accumulates. Physician surveys consistently identify administrative tasks performed outside of direct patient care as a leading driver of burnout, and pre-visit documentation review sits squarely in that category.
That does not make prospective capture the wrong choice. It makes physician workflow design the deciding variable. Organizations with well-integrated EHR systems, embedded pre-visit prep workflows, and strong MA or care coordinator support can absorb this burden without material attrition. Those without it should not assume the model will run itself.
Concurrent Capture and the Query Response Burden
Concurrent capture shifts burden from pre-visit preparation to post-visit query response. A physician who has already closed an encounter now receives a CDI query asking for clarification on a diagnosis, specificity upgrade, or condition linkage. Done well, this is a brief, high-value interaction. Done poorly, with high query volume, low clinical relevance, or poor query design, it becomes another administrative layer physicians resent.
Query fatigue is the primary failure mode for concurrent programs. Compliant query practice requires that queries be clinically grounded and non-leading, which means CDI programs relying on volume over quality will generate declining response rates over time. CMOs whose concurrent programs are generating response rates below 80 percent should treat that as a structural signal, not a physician compliance problem.
Why the Decision Depends on Your Contract Type and Population Mix
Medicare Advantage and MSSP Contracts
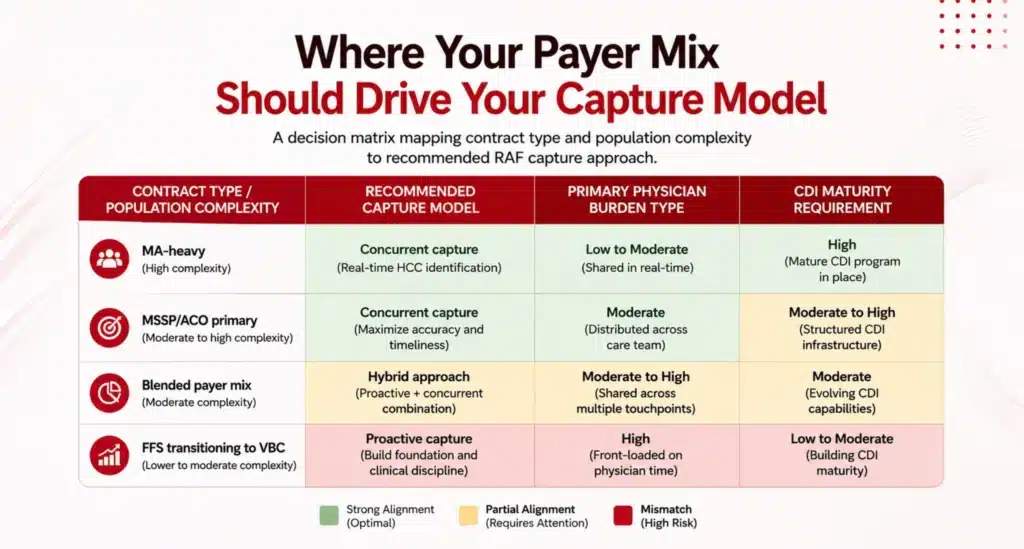
In Medicare Advantage, RAF accuracy determines your premium revenue directly. Undercoded HCCs produce RAF scores that underestimate your population’s acuity, and while CMS does provide mechanisms for supplemental data submission within defined windows, those pathways are narrow and operationally costly. For MA-heavy organizations, the argument for concurrent capture is strong: it catches documentation errors before claims close, and correcting them retroactively through supplemental submission is far more expensive than getting it right the first time.
MSSP participants face a different pressure. Your shared savings benchmark is set based on historical expenditures adjusted for risk, and your ability to stay below that benchmark determines whether you earn shared savings or owe losses. Prospective capture supports MSSP performance by ensuring your population’s acuity is accurately coded at the start of the measurement period, giving you a defensible baseline.
Complex and Medically Frail Populations
Consider populations with high comorbidity burdens: diabetics with chronic kidney disease, patients with multiple cardiovascular conditions, and patients with mental health and substance use comorbidities. These populations represent the highest RAF capture opportunity and the highest query complexity. A concurrent program staffed by general coders without CDI training underperforms badly in this context. CDI maturity is a precondition for concurrent capture, not a coincident factor.
Why Most Organizations Are Running a Blended Model Whether They Know It or Not
The prospective versus concurrent framing implies a binary choice. In practice, most health systems and medical groups are running a fragmented version of both: prospective HCC gap reports in some payer contracts, concurrent CDI review in inpatient settings, and neither functioning at full effectiveness in ambulatory VBC.
That fragmentation is not a strategy. It means your physicians are absorbing burden from two workflows without the organizational infrastructure to make either one efficient. It also means your RAF accuracy is inconsistent across your population, which creates the kind of HCC suppression that only becomes visible when a contract benchmark resets or a CMS audit surfaces underdocumentation patterns.
The CMOs who get this right are not choosing one model over the other. They are designing a capture program that allocates each approach to the population segment and contract type where it produces the best return at the lowest physician burden cost. That requires a clear view of your CDI maturity, your payer mix, and your EHR workflow capability, not a preference for one coding timeline over another.

Where Does Your Organization's RAF Capture Program Actually Stand?
If you are uncertain whether your current approach is prospective, concurrent, or an unplanned combination of both, that uncertainty is the answer. Most CMOs inherit RAF programs built for a different payer mix or a different contract structure, and the physician burden those programs generate often exceeds what the capture return justifies.
Download the Blended-Model Readiness Snapshot
The Blended-Model Readiness Snapshot is a one-page diagnostic for CMOs and VBC medical directors. It walks through where those gaps typically appear and identifies the highest-leverage interventions based on contract type, population mix, and CDI maturity.
DownloadFAQs
What Is the Difference Between Prospective and Concurrent RAF Capture?
Prospective RAF capture prepares HCC suspect lists before the encounter so physicians can address relevant conditions during the visit. Concurrent RAF capture reviews in-progress or recently completed charts and submits physician queries to correct or clarify documentation before the claim closes. Both improve RAF accuracy and HCC capture rate, but through different points in the clinical workflow and with different demands on physician time.
When Should a CMO Choose a Blended Capture Model Over a Single Approach?
A blended model makes sense when your payer mix includes both MA contracts, where concurrent capture protects closed-claim accuracy, and MSSP or ACO contracts, where prospective capture supports benchmark integrity at the start of the measurement period. Organizations with diverse contract structures and mixed population acuity almost always produce better RAF outcomes from a blended approach than from either model applied uniformly.
What Is a Healthy Physician Query Response Rate for a Concurrent CDI Program?
Industry benchmarks place compliant concurrent CDI programs in the 85 to 95 percent physician query response range. Programs below 80 percent warrant a structural review of query design, query volume, and CDI staff training. The operational fix usually involves tightening query targeting so physicians only receive queries with material clinical or financial impact.
The Capture Model Is a Clinical Workforce Decision
Prospective and concurrent RAF capture are not interchangeable tools. Each places a different kind of demand on your physicians, at a different point in the care cycle, and against a different contract performance objective. The CMOs who build durable RAF programs treat the capture model selection as an organizational design decision, one that accounts for CDI maturity, payer contract structure, population complexity, and the physician workforce’s actual capacity to absorb documentation burden.
The question is not which approach is better. The question is which approach your organization is actually set up to run well, and where the gaps between your current program and that standard are costing you accuracy, revenue, or provider satisfaction.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. I've led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let's connect to modernize workflows.