





















What CMOs at Top-Performing ACOs Do Differently
The CMOs running the highest-performing ACOs are not reading a quality report and reacting. They have built the clinical governance structures, documentation workflows, and physician feedback loops that make the report a formality rather than a surprise. Based on Chirok Health’s work with ACO leadership teams, that infrastructure takes 12 to 18 months to build. The results look like a sudden performance leap from the outside. They are not sudden.
If your ACO is missing its shared savings benchmark, struggling with HCC capture rates, or watching quality scores plateau, the gap is almost certainly upstream of the data. Top ACOs are built before the report lands. This post breaks down the specific operating differences between CMOs producing those results and those managing reactive cycles year after year. The differences are structural, not philosophical.
Why Most ACO CMOs Are Solving the Wrong Problem
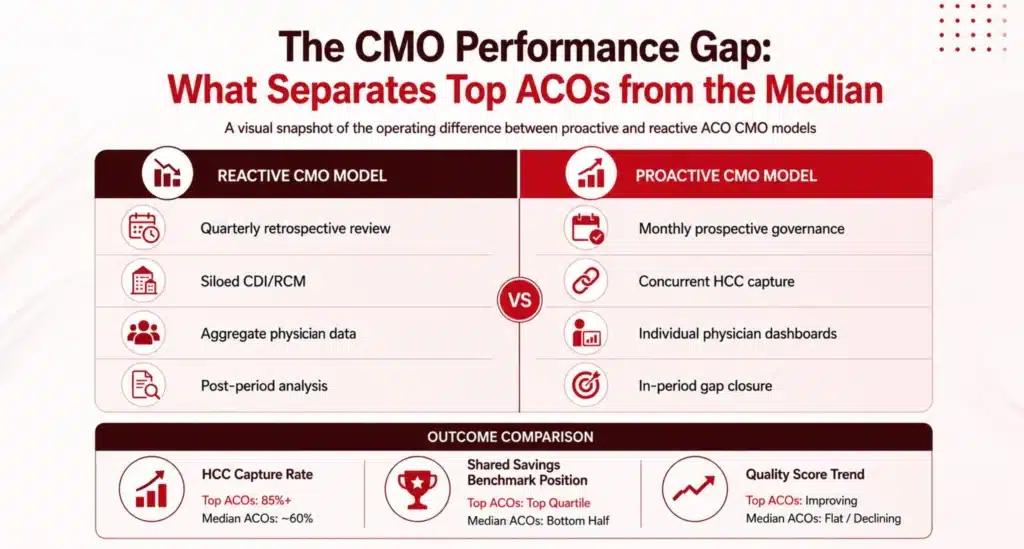
Most ACO CMOs spend the bulk of their bandwidth on quarterly performance reviews, payer contract negotiations, and responding to utilization outliers after they have already affected the benchmark. These are real responsibilities. But they are downstream of the decisions that actually determine ACO performance. A CMO who spends the majority of their time on retrospective analysis is not building the infrastructure that prevents the problem next cycle.
The diagnostic question is not “how is our ACO performing?” It is “where in the care cycle are we losing credit for the work we are already doing?” CMOs at top-performing ACOs can answer that question specifically: which HCC diagnoses are being missed at the point of encounter, which quality gaps are closing too late in the performance year, and which physicians have documentation patterns that suppress risk adjustment accuracy. CMOs at median-performing ACOs typically cannot.
The gap is not clinical. It is operational. It comes down to whether the CMO has built a system that acts on data in real time or one that reviews it quarterly after the window to act has closed.
What the Operating Model Looks Like at Top-Performing ACOs
High-performing ACO CMOs share a common structural approach. They separate the functions of clinical quality oversight, risk adjustment accuracy, and care coordination into distinct workflows with distinct owners, rather than collapsing everything under a single quality umbrella. Each function runs on its own data cadence and has its own feedback loop to the physician level.
Clinical Governance That Runs Between Reporting Periods
Top CMOs hold monthly clinical governance reviews that are not performance postmortems. They are prospective: which care gaps are still open for high-risk attributed patients, which HCC diagnoses are insufficiently documented for the current encounter period, and which physicians have query response rates that need attention. The review exists to close gaps before the performance period ends, not to explain why they were missed after the fact.
ACOs with structured concurrent documentation review programs consistently outperform those relying on retrospective audit cycles alone on HCC capture rates. The mechanism is straightforward: a coder or CDI specialist reviewing an in-progress chart can prompt a physician to document a diagnosis that is clinically present but absent from the record. That same prompt, sent six months after the encounter, cannot recover the revenue or the quality credit.
Physician Feedback That Changes Behavior, Not Just Awareness
The second structural difference is how CMOs use physician-level performance data. In median-performing ACOs, physicians receive an annual or semi-annual summary of their quality metrics. In top-performing ACOs, physicians see a monthly dashboard showing their individual HCC capture rate, care gap closure rate by condition, and estimated contribution to the ACO’s shared savings benchmark. The data is specific enough to act on and delivered frequently enough to change behavior before the performance cycle closes.
This is not a performance exercise. A physician who knows their diabetic patient’s HCC for chronic kidney disease is not captured in the current record will document it. A physician who finds out six months later that it was missing will not have the opportunity to fix it. The feedback loop is the intervention. Its value comes from timing.
The Financial Levers CMO Strategy Actually Controls
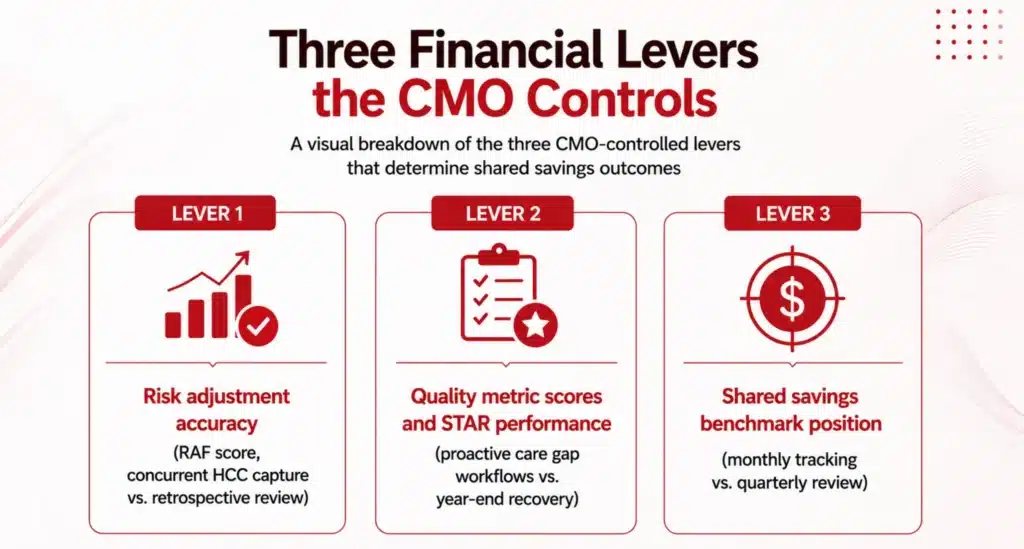
ACO CMO leadership is often framed in terms of quality outcomes. That framing is accurate but incomplete. The CMO’s operating model directly controls three financial levers that determine whether the ACO achieves shared savings and how much.
Risk Adjustment Accuracy
In a Medicare Advantage or MSSP context, your risk adjustment accuracy determines your benchmark. An ACO with a suppressed RAF score is operating against a benchmark that makes shared savings structurally harder to achieve, regardless of how well care is managed. CMOs at top-performing ACOs treat RAF integrity as a clinical operations problem, not a coding problem. They embed concurrent HCC capture into the encounter workflow rather than relying on retrospective chart review to recover missed diagnoses after the fact. With V28’s coefficient changes and dropped codes now in effect, the margin for retrospective recovery has narrowed further, making concurrent capture more consequential for benchmark integrity than it has been in any prior model year.
Quality Metric Scores and STAR Performance
HEDIS and STAR measures are a direct output of whether your care coordination model is closing gaps consistently across your attributed population. CMOs who build proactive care gap workflows, where a patient’s open measures are surfaced to the care team before the encounter rather than after, produce higher STAR scores than those relying on year-end outreach campaigns to recover missed measures. The difference is structural, not effort.
Shared Savings Benchmark Position
The shared savings benchmark is set before the performance year begins. CMOs who understand the mechanics of their MSSP Track or Enhanced Track agreement know exactly how much of their attributed population’s spend needs to come in under benchmark for the ACO to generate savings. That number drives decisions about care management resource allocation, high-risk patient identification, and post-acute utilization management. CMOs at top performers track it monthly. Most others track it quarterly at best, which leaves too little time to respond when the trajectory is off.
How to Build the Internal Business Case
The business case for restructuring CMO operations around proactive clinical governance starts with three questions: What is your current RAF score versus your estimated optimal score based on your population’s documented comorbidity burden? What is your HCC capture rate versus the top-quartile benchmark for your ACO peer group? And what has your shared savings position been over the last two performance years?
The answers to those three questions usually reveal a recoverable gap. An ACO that is undercapturing HCC diagnoses is leaving benchmark credit on the table for conditions its physicians are already managing. The cost of closing that gap, through concurrent CDI staffing, physician feedback infrastructure, and data integration, is typically a fraction of the benchmark improvement it produces. The math depends on your specific contract structure and baseline capture rates, but the direction is consistent: organizations that shift from retrospective to concurrent documentation review capture more of what they have already earned.
What the Organizational Model Needs to Look Like
CMO Oversight of CDI and RCM Workflow
CDI and the revenue cycle functions that depend on it need to coordinate with the CMO’s office, not operate as parallel functions under separate leadership. This does not require a reorganization. It requires a formal governance structure, shared data, and a standing monthly review where CDI performance is treated as a clinical quality metric, not a compliance or billing metric.
A Concurrent Coding and Care Gap Function Embedded in Care Management
Retrospective coding review should not be the primary mechanism for HCC capture. CMOs at top-performing ACOs have built or contracted concurrent workflows where certified coders and CDI specialists review in-progress charts for high-risk attributed patients, identify missing diagnoses, and route queries to the physician before the encounter closes. This function sits inside care management, not in a back-office coding team.
Physician Feedback Infrastructure with Clear Accountability
Monthly individual-level dashboards are not sufficient on their own. They need a structured response mechanism: a process by which physicians with low HCC capture rates or care gap closure rates are contacted by a clinical coordinator, not a billing department, and given specific guidance on what documentation is missing and why it matters for the patient’s care plan. The clinical framing matters. Physicians respond to it differently than administrative outreach.

Where Does Your Organization Stand on Blended-Model Readiness?
Most ACOs have made progress on the data side: better attribution reporting, cleaner dashboards, more granular quality metrics. Fewer have built the operational infrastructure on the clinical side that turns data into action before the performance period ends. The gap between those two states is where shared savings are lost.
Chirok Health works with ACO leadership teams to assess the maturity of their clinical governance infrastructure, identify where HCC capture and quality gap closure are breaking down, and build the operating model that closes those gaps. The starting point is understanding precisely where your organization sits relative to top-performing ACO benchmarks.
Download the Blended-Model Readiness Snapshot
The Blended-Model Readiness Snapshot is a one-page diagnostic for CMOs and VBC medical directors. It walks through where those gaps typically appear and identifies the highest-leverage interventions based on contract type, population mix, and CDI maturity.
DownloadFAQs
What Is the Difference Between ACO CMO Leadership and Traditional CMO Responsibilities?
A traditional CMO role centers on credentialing, clinical quality events, and medical staff governance. ACO CMO leadership adds a different operating layer: prospective management of attributed population risk, concurrent HCC capture oversight, and direct accountability for shared savings benchmark performance. The difference is not about clinical expertise. It is about whether the CMO's operating model is built for retrospective quality assurance or for real-time clinical governance across a defined population.
How Does Risk Adjustment Accuracy Connect to ACO Quality Outcomes?
Risk adjustment accuracy determines the benchmark against which your ACO's spending is measured. An underweighted RAF score artificially lowers your benchmark, making shared savings harder to achieve regardless of how efficiently care is managed. ACOs that improve risk adjustment accuracy through concurrent HCC capture see a direct improvement in shared savings position because the benchmark more accurately reflects the clinical complexity of their attributed population. The quality outcomes follow because concurrent documentation review also surfaces care gaps that would otherwise go unaddressed.
When Should an ACO CMO Bring in an External CDI Partner Versus Building Internally?
Build internally if your CDI program already has concurrent capabilities, your EHR infrastructure supports real-time coding queries, and you have the staffing pipeline to sustain it. Partner externally if your program is primarily inpatient-centric, your payer mix is shifting faster than your internal capacity can adapt, or you need to show shared savings improvement within the 12-to-18-month window that Chirok Health typically sees in client engagements. External CDI partners with ACO-specific experience can compress a build timeline significantly because the workflow design, physician engagement model, and coding infrastructure already exist.
The Gap Closes Before the Quality Report, Not After
Top-performing ACO CMOs are not reading a better quality report. They built a different operating model in the 12 to 18 months before that report landed. The clinical governance structure, the concurrent HCC capture workflow, the physician feedback infrastructure, and the CDI and RCM alignment under CMO oversight are the inputs that produce top-quartile results. They are also the inputs that most median-performing ACOs have not fully built.
The starting point is an honest assessment of where your current model stands against those benchmarks. Once you know the specific gaps, the path to closing them is operationally clear.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. I've led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let's connect to modernize workflows.