





















What Actually Changed When a Health System Moved to Value-Based Care
The gap between health systems that succeed in value-based care and those that stall is rarely a care delivery gap. Clinicians at both kinds of organizations are largely doing the same work. What separates them is what their organizations knew about their patients before the contract started: how completely the documentation captured complexity, how accurately the risk scores reflected acuity, and whether physician feedback loops were in place from day one.
Quality scores move. Utilization patterns shift. Revenue timing changes. The trajectory of all three is set in the first twelve months, and it is set by infrastructure decisions most leadership teams underestimate going in. Where specific outcome data appears below, it is drawn from client work with a large academic health system in the Northeast operating across fee-for-service and value-based contracts.
Documentation Accuracy at Contract Entry Shapes Everything That Follows
Organizations entering VBC contracts with stronger baseline documentation accuracy outperform peers on risk-adjusted quality metrics within 24 months. Not because their clinicians deliver different care. Because their documented patient complexity more accurately reflects the population they are being asked to manage.
Clinical quality improvements in VBC are not evenly distributed. Ambulatory chronic disease management (diabetes, hypertension, COPD) shows measurable change within the first year when care gap closure workflows are in place. Inpatient metrics respond more slowly.
With this client, the concurrent documentation workflow surfaced social needs the formal screening tool was consistently missing. Transportation barriers, food access, housing instability: conditions that registered as negative on the structured SDoH screen began appearing in physician visit notes once the workflow prompted clinicians to capture context the screening questions did not. The screening process was finding the patients. The documentation workflow was finding the conditions. That distinction matters: risk-adjusted quality metrics in value-based contracts depend on what is documented, not what is asked.
Without an accurate baseline, year-one quality scores reflect what was already known. Which is rarely enough.
The Financial Mechanics Catch Leadership Teams Off Guard
In FFS, an organization bills for what it does. In VBC, revenue is calibrated against what the organization was expected to do for a population with a specific risk profile. When that risk profile is understated at benchmark-setting, the contract period is spent chasing a target that does not reflect the patients.
Risk Adjustment Accuracy at Contract Entry
The risk adjustment factor (RAF) for a Medicare Advantage or Medicare Shared Savings Program (MSSP) population is calculated from historical claims and encounter data. If hierarchical condition category (HCC) capture has been running below actual patient complexity, the benchmark set at contract entry will understate the population. A health system entering VBC with a significant HCC capture gap starts in a structural deficit care delivery alone cannot recover.
For the same client, RAF scores rose 32% in the first 18 months after concurrent capture replaced retrospective review. Work RVU performance climbed 26 to 28% over the same period. The two outcomes were not separate effects of two separate programs. They were the same effect, accurate documentation surfacing clinical complexity that had been invisible to the prior workflow, measured through two different lenses.
Shared Savings Benchmark Integrity
Shared savings compares actual expenditures against a risk-adjusted benchmark. If documented complexity is lower than true acuity, the benchmark is too low and the savings position shrinks even when care is being managed well. The difference is not in care delivery. It is in when and how completely diagnoses are documented.
Quality Incentive Eligibility is Binary
Most VBC contracts include quality incentive thresholds tied to HEDIS or STARS measures. Missing those thresholds by a small margin forfeits incentive payments entirely, not proportionally. For a $200 million value-based book, that can mean $6 to $12 million in payments contingent on quality score precision, not care quality alone.
At the documentation query volume the program runs, it adds approximately one HCC for every 60 queries. The incremental revenue per encounter ranges from $5 to $50 depending on encounter type, on top of what retrospective coding had captured. The numbers are not dramatic on a per-encounter basis. The point is that they compound consistently across the full population, month after month, in a way that retrospective workflows could not.
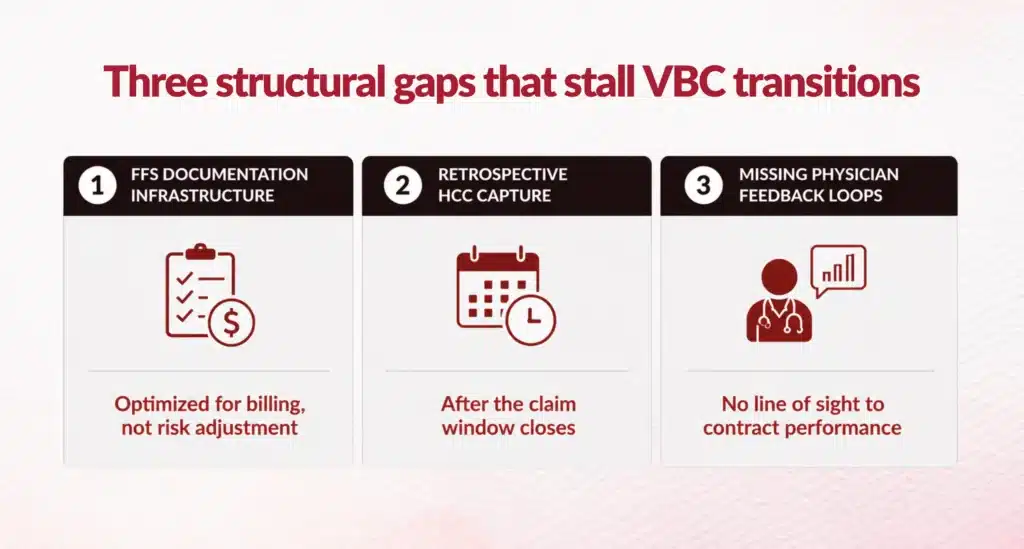
Three Structural Gaps Stall Most VBC Transitions
Underperforming transitions share three structural problems. Spotting them early beats discovering them through two years of performance data.
Documentation Infrastructure Designed for Fee-For-Service
FFS documentation is optimized for billing accuracy at the encounter level. VBC documentation needs longitudinal patient complexity, chronic condition specificity, and the hierarchical condition categories that drive risk adjustment. Most electronic health records (EHRs) are not configured for the latter by default. Physicians who documented accurately for FFS for years can be systematically underdocumenting for VBC without any change in behavior.
Retrospective HCC Capture Misses the Window
Retrospective coding works after the claims window has closed. Diagnoses missed at the point of care and not corrected before claim submission do not improve risk score or shared savings benchmark. Concurrent clinical documentation integrity (CDI) programs address this gap at the source.
Physician Engagement Without Feedback Loops
Physicians in VBC arrangements are often asked to document differently without being shown why or how it affects contract performance. Query volumes go up, response rates go down, and the documentation gap widens. The organizations that close the gap fastest give physicians monthly dashboards: individual HCC capture rate, query response rate, estimated contribution to shared savings position.
Where Does Your Organization Stand on the VBC Transition?
Most health systems in VBC contracts know their quality scores and their shared savings position. Fewer have clear visibility into the documentation gaps, HCC capture rates, and benchmark accuracy issues shaping those numbers. The fix is well documented at this point. The question is whether you can see, in your own organization, where the gaps actually sit.
Download the Blended-Model Readiness Snapshot
The Blended-Model Readiness Snapshot is a one-page diagnostic for CMOs and VBC medical directors. It walks through where those gaps typically appear and identifies the highest-leverage interventions based on contract type, population mix, and CDI maturity.
Download
The Data is There for Organizations Willing to Look at It Clearly
The gap between organizations that improve in VBC and those that stall is not primarily a care delivery gap. It is a documentation accuracy gap, a risk adjustment timing gap, and a physician feedback gap. Health systems that close those three in the first 12 months of a VBC contract enter year two from a fundamentally different position than those that do not. The interventions are known. The starting point is an honest read of where the documentation baseline actually stands.
FAQs
1. How do I know if our documentation baseline is the constraint versus our care delivery?
The clearest signal is a mismatch between your quality scores and your shared savings position. If your HEDIS or STARS performance is improving but your shared savings position is not moving proportionally, care delivery is not the problem. Your documented patient complexity is understating actual acuity, which suppresses your benchmark and narrows your savings corridor regardless of how well you manage the population. A second signal is RAF score stability over two or more contract years despite population growth. Flat RAF in a growing, aging population means documentation is not keeping pace with clinical reality.
2. What is the realistic cost of waiting another year to fix HCC capture?
On a $200 million value-based book, a 10-point HCC capture gap running for 12 months represents a suppressed benchmark that cannot be retroactively corrected once the contract period closes. The compounding effect is the part most leadership teams underestimate: a low RAF at contract entry sets a low benchmark, a low benchmark shrinks the shared savings corridor, and a narrow corridor limits recovery even when utilization improves in year two. The cost is not one year of lost revenue. It is a baseline that resets your starting position for the next contract negotiation.
3. How long does it take to see financial results after moving from retrospective to concurrent HCC capture?
For the academic health system referenced in this post, RAF scores rose 32% within 18 months of replacing retrospective review with concurrent capture. The first measurable movement typically appears at the six-month mark, when enough encounters have run through the new workflow to shift the documented risk profile. The financial translation, shared savings position and quality incentive eligibility, follows the RAF movement by one to two quarters depending on how your payer calculates mid-year adjustments.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. I've led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let's connect to modernize workflows.