





















The VBC Metrics a CMO Should Govern, and the Ones That Are Just Noise
Most CMOs in value-based care contracts have seen the same problem: a dashboard that grows with every contract renewal until it covers 40 or 50 metrics, and a governance agenda that tries to address all of them. The result is not oversight. It is noise management.
Separating CMO governance from operational reporting is not a matter of preference. In Medicare Advantage and MSSP contracts, a small set of measures drives the majority of contract performance. Your governance seat belongs on those measures. This post identifies which ones they are, why the rest do not belong in your weekly review, and what the cost of dashboard sprawl actually looks like.
Governance metrics differ from operational ones in one specific way: leverage
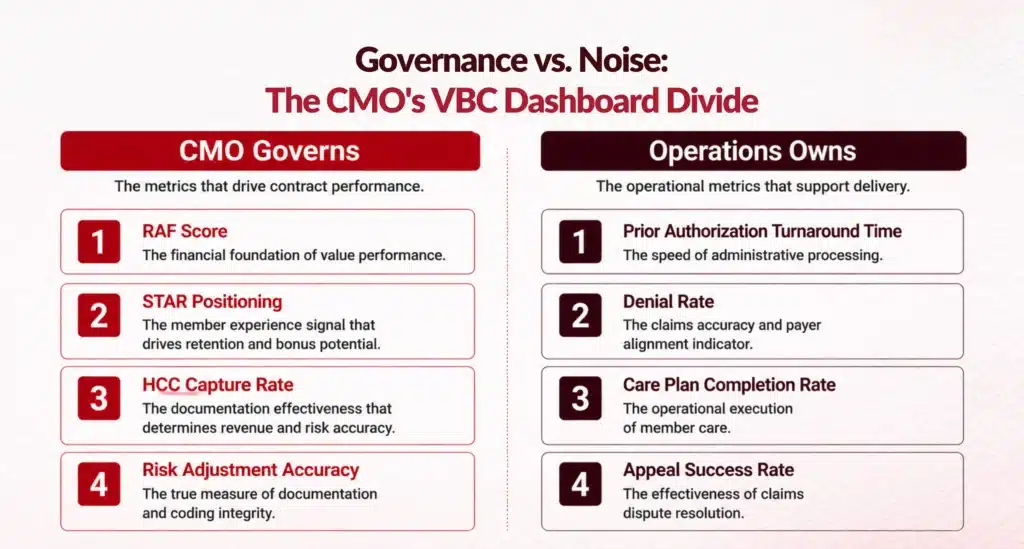
The distinction is not complexity or volume. A governance metric is one where your decision directly changes the outcome, where the financial or quality stakes warrant executive attention, and where delay compounds the problem. An operational metric is one where the right response is a process fix or a threshold alert your team can own.
A useful test: if the metric does not change what you would decide, approve, or escalate this quarter, it does not belong on your governance agenda. By that test, three categories meet the threshold in value-based care: risk adjustment accuracy, quality measure performance in high-stakes domains, and contract benchmark positioning. Everything else is operational data.
The three metrics that belong in your governance seat
RAF score accuracy and HCC capture rate
STAR and HEDIS performance in high-weighted domains
Not every HEDIS measure belongs in your governance review. Your oversight should focus on the measures with the highest point weight in your STAR rating and the largest current gap. For most MA contracts, that means Medication Adherence, Diabetes Care, and Controlling High Blood Pressure. You govern the measure-level position and approve the interventions. Your team tracks execution against specific patient cohorts and network providers.
Shared savings benchmark positioning
In MSSP ACO contracts, if your RAF scores are understated, your benchmark is set too low, and you enter each performance year at a structural disadvantage regardless of how well your care teams manage utilization. CMOs who govern only utilization and not risk adjustment accuracy often find their ACO finishes within budget but misses the shared savings corridor because the benchmark was wrong from the start.
The metrics that crowd CMO agendas without earning the seat
This is not an argument that operational metrics are unimportant. It is an argument that the wrong person reviewing the right data still produces the wrong outcome. Three categories consistently crowd CMO governance agendas without requiring a CMO-level decision.
Claim denial rates and prior authorization turnaround are revenue cycle metrics. They affect cash flow and administrative burden and belong with your RCM team.They reach you only when they create access barriers that affect quality measures or patient safety.
Care management platform engagement statistics (logins, outreach attempts, care plan completion rates) are process metrics. They tell you whether your team is doing the work, not whether the work is producing outcomes. The outcome metric that follows, gap closure rate on high-stakes HEDIS measures, is what belongs on your agenda.
Provider-level productivity and scheduling throughput matter for revenue and access planning but do not drive VBC contract performance directly. They surface to you only when a specific provider’s documentation patterns are suppressing HCC capture at scale, which is a different question than throughput.
Why dashboard sprawl is a latency problem, not a cognitive load problem
Dashboard expansion follows contract expansion. Each new payer contract comes with reporting requirements that accumulate in whatever governance structure already exists. Within two or three cycles, a CMO dashboard built for a single MSSP agreement is carrying MA STAR data, commercial measures, state Medicaid metrics, and FFS RCM benchmarks simultaneously.
The cost is not just attention. It is latency. When every metric is a governance metric, the ones that require an actual decision get the same two minutes of meeting time as the ones that are simply informational. The governance gaps that produce contract underperformance are not visible in a single quarter. They show up in RADV audit outcomes, in benchmark integrity at renewal, and in whether your organization enters each performance year with an accurate risk profile or an inherited disadvantage.
Where does your organization stand on VBC governance?
Many CMOs recognize the dashboard problem but are unsure where to start restructuring. The challenge is that governance gaps are not always visible in performance data until a contract cycle has already closed. By then, the revenue implication is locked in.
The Blended-Model Readiness Snapshot is a one-page diagnostic for CMOs and VBC medical directors. It walks through where these gaps typically appear and identifies the highest-leverage interventions based on contract type, population mix, and CDI maturity.
Download the Blended-Model Readiness Snapshot
The Blended-Model Readiness Snapshot is a one-page diagnostic for CMOs and VBC medical directors. It walks through where those gaps typically appear and identifies the highest-leverage interventions based on contract type, population mix, and CDI maturity.
Download

FAQs
What Is the Difference Between a Governance Metric and an Operational Metric in VBC?
A governance metric is one where the CMO's decision directly changes the outcome and where the financial or quality stakes are high enough to warrant executive attention. In value-based care, governance metrics include RAF score accuracy, HCC capture rates, and STAR measure performance on high-weighted domains. Operational metrics, such as prior authorization turnaround times and care plan completion rates, require process management rather than clinical governance decisions.
Which HEDIS Metrics Should a CMO Actively Govern?
CMO governance should focus on the HEDIS measures with the highest point weight in your STAR rating and the largest current gap against your benchmark population. For most Medicare Advantage contracts, that includes Medication Adherence across diabetes, hypertension, and cholesterol drug classes, Diabetes Care measures, and Controlling High Blood Pressure. Annual NCQA HEDIS benchmarks help identify which performance gaps are large enough to influence STAR ratings.
How Does RAF Score Accuracy Affect MSSP Benchmark Positioning?
In MSSP ACO contracts, benchmarks are calculated using historical expenditures adjusted for patient acuity reflected in RAF scores. If chronic conditions are underdocumented and RAF accuracy is low, the benchmark is established below the organization's actual patient complexity. This creates an artificially low spending target, making shared savings significantly harder to achieve even when care management performance is strong.
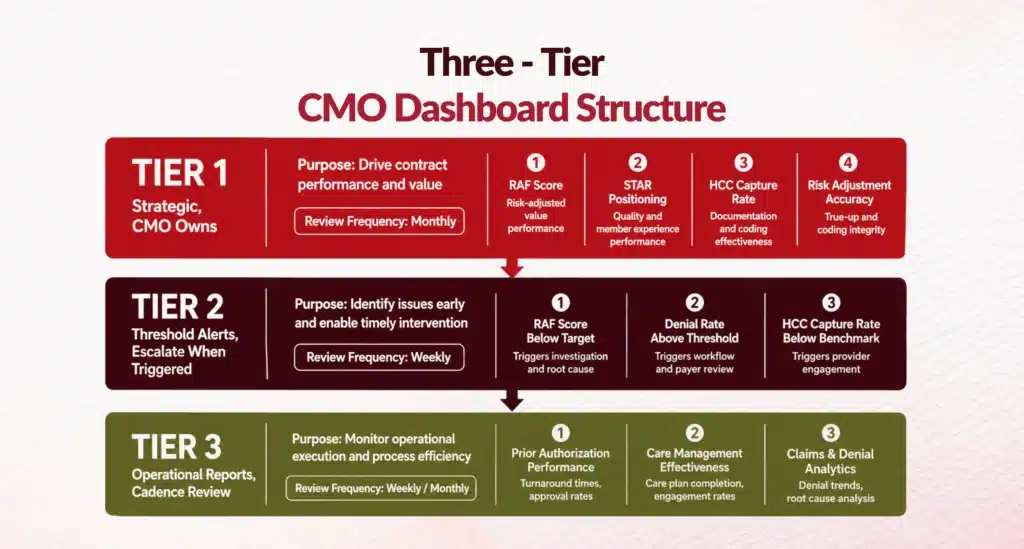
How Often Should a CMO Review Their VBC Performance Dashboard?
Strategic value-based care metrics should be reviewed weekly or every two weeks during active contract performance periods, with threshold-based alerts escalated immediately when triggered. Operational reports, including utilization trends, denial rates, and care management engagement, can typically be reviewed monthly. The objective is to make governance decisions while they can still influence contract outcomes rather than after the performance period ends.
What Are the Risks of Leaving RAF Score Gaps Unaddressed?
Inaccurate or undercoded RAF scores create both financial and compliance risk. They reduce per-member-per-month reimbursement in Medicare Advantage because payment is based on documented risk rather than clinical complexity. They also increase RADV audit exposure if unsupported HCC diagnoses are identified, potentially resulting in repayment obligations covering multiple contract years. Maintaining documentation accuracy is therefore both a revenue and governance priority.
When Should a CMO Restructure Their Governance Dashboard?
Governance dashboards should be restructured before contract renewal cycles, allowing organizations to establish meaningful baseline metrics for upcoming agreements. A clear indicator that redesign is needed is when leadership meetings spend most of their time reviewing operational statistics rather than making governance decisions. Effective dashboards prioritize actionable contract metrics over excessive reporting, enabling faster executive decision-making and stronger value-based performance.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. I've led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let's connect to modernize workflows.