



















RADV Readiness Is a Documentation Integrity Problem, Not a Compliance One
Most Medicare Advantage organizations treat RADV readiness as a compliance function. The auditors arrive, compliance responds, clinical staff get pulled in after the fact. That structure almost guarantees the outcome you are trying to avoid. RADV audits do not fail because compliance teams are unprepared. They fail because the documentation underlying your HCC submissions was never built to survive chart-level scrutiny.
If you lead clinical operations for a Medicare Advantage plan or risk-bearing medical group, this is your problem to own. The physicians coding your highest-acuity members answer to you. The CDI workflows supporting HCC capture run through your organization. RADV exposure is a documentation integrity problem, which makes it a clinical leadership problem.
What RADV Actually Tests
RADV audits sample the HCC codes a plan submits for payment and check whether the underlying medical records support them. CMS has the authority to extrapolate audit findings across the full plan population, not just the audited sample. When a sample shows a meaningful error rate, that error rate applied across thousands of member-years produces large repayment demands. This is not a documentation review. It is a financial settlement process.
The error most organizations make is conflating RADV readiness with coding accuracy. Coding accuracy is necessary but not sufficient. RADV tests whether every submitted HCC is supported by documentation that meets CMS specificity standards in a specific date-of-service record. A condition can be clinically real and still fail RADV if the note does not document it to the required specificity, in the right place, signed by a qualified provider.
Where Documentation Gaps Actually Originate
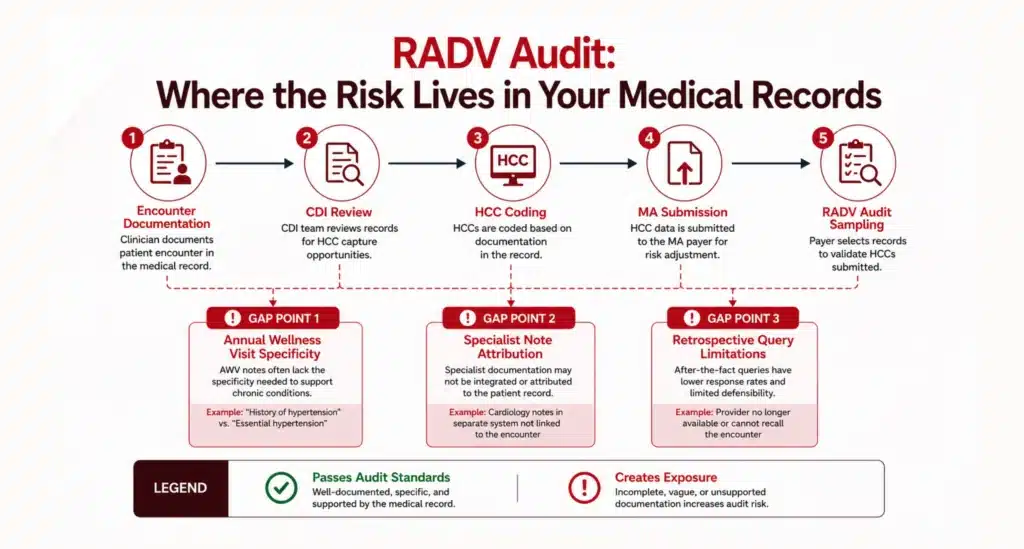
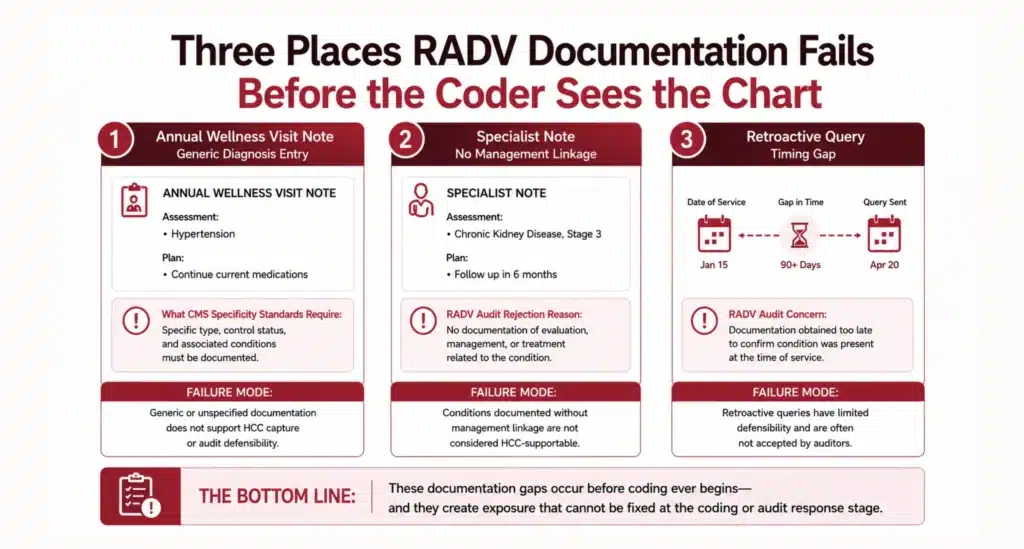
RADV exposure does not accumulate at the coding stage. It accumulates at the encounter. By the time a coder touches a chart, the documentation is already fixed. Gaps concentrate in three predictable places.
Annual wellness visits structured for HEDIS, not risk adjustment
Annual wellness visits are the primary HCC capture vehicle in many MA populations, but many are structured to satisfy HEDIS metrics rather than document chronic conditions at the specificity CMS requires. A note recording a diagnosis code without describing the clinical basis, current status, and management plan will not hold up under RADV review.
Specialist notes that miss linkage language
High-acuity HCCs often rest on specialist documentation. Cardiology, nephrology, endocrinology notes written for a clinical audience frequently omit the linkage language a risk adjustment submission requires. The cardiologist documents heart failure. The note does not specify systolic versus diastolic, current functional status, or acknowledgment of ongoing management. The HCC gets submitted. The auditor finds the note insufficient.
Retroactive queries that look like audit response
CMS RADV protocols are skeptical of addenda and late amendments appearing in response to audit activity. Documentation not in the original chart, at the time of service, from the treating provider, faces a higher bar. Retrospective queries can address some gaps but cannot substitute for documentation built correctly at the point of care.
Why This Is a CMO Problem, Not a Compliance Problem
Compliance officers can identify RADV exposure after it exists. They cannot prevent it at the source. The documentation culture determining whether your HCCs are audit-defensible is set at the clinical leadership level. It lives in how you structure annual wellness visits, how you query specialists, how you train physicians on documentation expectations, and whether CDI has clinical authority or operates as a back-office function.
The OIG has consistently flagged Medicare Advantage as a focus area for payment accuracy oversight, with diagnosis codes submitted without adequate medical record support cited as a recurring source of improper payments. The integrity problem is not theoretical. It is documented at the federal level as systemic across the MA program.
CMOs who own this treat it as a clinical quality issue: are our physicians documenting the conditions they are managing at the specificity those conditions require? CMOs who do not own it discover during an audit that their plan has been billing for risk it cannot defend.
Where does your organization stand on RADV readiness?
Most CMOs and VBC medical directors know there are documentation gaps in their risk-bearing contracts. Fewer have a clear picture of where those gaps concentrate, how they map to their specific population and contract structure, or which interventions would produce the most improvement before an audit cycle begins. The fix is well understood at this point. The question is whether you can see, in your own organization, where the gaps actually sit.
The Blended-Model Readiness Snapshot is a one-page diagnostic for CMOs and VBC medical directors. It walks through where these gaps typically appear and identifies the highest-leverage interventions based on contract type, population mix, and CDI maturity.
Download the Blended-Model Readiness Snapshot
The Blended-Model Readiness Snapshot is a one-page diagnostic for CMOs and VBC medical directors. It walks through where those gaps typically appear and identifies the highest-leverage interventions based on contract type, population mix, and CDI maturity.
DownloadFAQs
What Is the Difference Between a RADV Audit and a Routine Coding Audit?
A routine coding audit typically checks whether the diagnosis codes submitted match the documentation in the chart. A RADV audit goes further: it tests whether CMS's specific documentation requirements for risk adjustment are met, including the provider type, date of service, condition specificity, and linkage language. A condition can be correctly coded and still fail RADV audit standards if the underlying note does not meet CMS documentation criteria for HCC documentation accuracy.
How Does CMS Select Which Plans and Members Are Audited?
CMS selects MA organizations for RADV audits using a combination of plan-level risk factors and statistical sampling methods. Within a selected plan, CMS draws a random sample of enrollees and requests medical records for the HCC diagnoses submitted for those members in a contract year. The audit is a retrospective review of whether the submitted diagnosis codes are supported by medical records from that payment year.
Can Retrospective Queries Fix RADV Documentation Gaps?
Retrospective queries can address some gaps, particularly where a condition was genuinely documented but the specificity language was missing. They cannot create documentation that did not exist at the time of service, and CMS RADV audit protocols treat late addenda with scrutiny, particularly those generated in proximity to an audit. The stronger intervention is prospective CDI: closing gaps before the claim is submitted rather than attempting to correct them after the fact.
What HCC Categories Carry the Highest RADV Audit Risk?
High-acuity HCC categories with complex specificity requirements carry the most documentation risk: heart failure (systolic vs. diastolic, chronic vs. acute), diabetes with complications, chronic kidney disease staging, and major depressive disorder. These are also among the highest-weighted HCCs in the CMS risk adjustment model, which is why documentation errors in these categories produce the largest financial exposure in a RADV audit.
What Organizational Changes Does CMO-Led RADV Readiness Require?
CMO-led RADV readiness typically requires three structural changes: moving CDI from a retrospective audit function to a concurrent clinical program with physician access; building physician feedback loops that give providers visibility into their own HCC documentation rates; and elevating documentation standards from compliance guidance to clinical policy. The last item is the one that requires CMO authority. Compliance departments can recommend documentation standards. CMOs can enforce them.
How Long Does It Take to Materially Improve RADV Audit Defensibility?
Organizations that implement concurrent CDI with physician feedback loops typically see measurable improvement in HCC documentation accuracy within two to three contract quarters. RADV audit defensibility is a function of the documentation in the medical record at the time of service. Improvements you make now apply to the current payment year's HCC submissions. The lag is real, but the improvement compounds: a stronger documentation culture in year one reduces exposure in year two and beyond.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. I've led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let's connect to modernize workflows.