





15 Common Documentation Gaps Found in Payor Retrospective Reviews
Why Retrospective Reviews Are Exposing Critical Documentation Breakdowns
Healthcare payors today operate in an audit-intensive environment where retrospective reviews directly influence RAF accuracy, compliance exposure, and financial performance. If you lead Risk Adjustment or Provider Network Management, you already know this reality: most audit failures aren’t driven by coding alone; they stem from documentation gaps.
Industry reviews show that nearly 50% of coding errors originate from insufficient or missing provider documentation. With CMS accelerating RADV audits and expanding retrospective scrutiny, unsupported diagnoses can trigger repayment, penalties, and reputational risk.
This blog answers the core question first, what documentation gaps payors most commonly uncover, and then dives deeper into root causes, operational impact, and mitigation strategies.
What Are the Most Common Documentation Gaps Identified in Retrospective Payor Reviews?
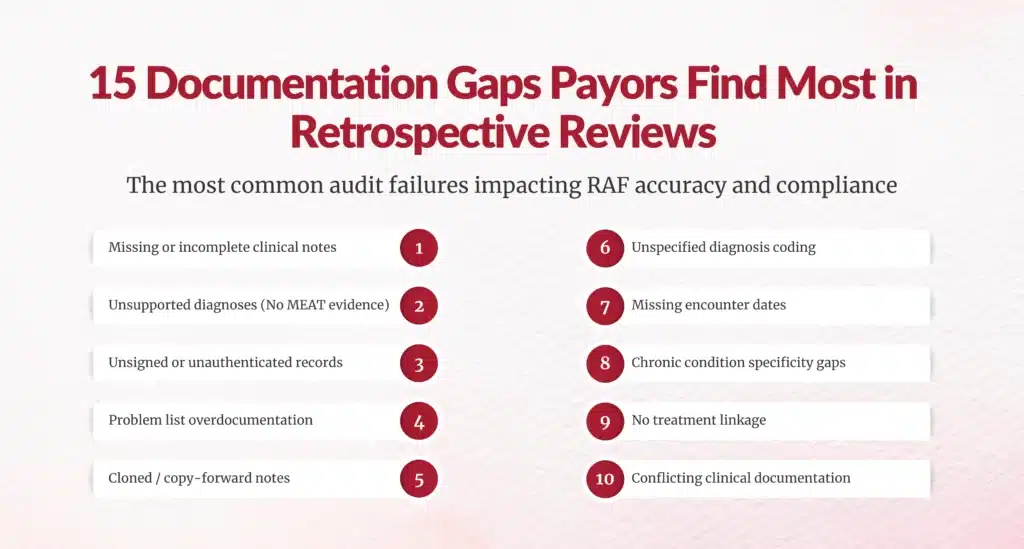
Below are the 15 documentation deficiencies most frequently flagged during retrospective audits, RADV validations, and risk adjustment chart reviews.
1. Missing or Incomplete Clinical Notes
Encounters lacking full visit documentation remain the top audit trigger. Missing histories, assessments, or plans make diagnoses unverifiable.
2. Diagnoses Without Assessment or Treatment Evidence
Conditions must show active monitoring, evaluation, or management (MEAT criteria). Unsupported diagnoses are routinely invalidated.
3. Lack of Provider Signature or Authentication
Unsigned notes or missing credentials automatically fail audit validation.
4. Missing Encounter Dates
Undated documentation cannot confirm service timelines or risk capture periods.
5. Unsupported HCC Coding
Hierarchical Condition Categories must be backed by clinical specificity and evidence.
6. Overreliance on Problem Lists
Problem lists alone do not confirm active management and are frequently rejected.
7. Copy-Forward or Cloned Documentation
Cloned notes without patient-specific updates create compliance red flags.
8. Incomplete Chronic Condition Specificity
Auditors downgrade vague diagnoses lacking severity, stage, or complications.
9. Missing Linkage Between Conditions and Treatment Plans
Clinical documentation must connect diagnoses to medications, labs, or care plans.
10. Use of Unspecified Diagnosis Codes
Non-specific ICD-10 codes reduce RAF validity and audit acceptance.
11. Lack of Face-to-Face Encounter Evidence
Risk-adjustable diagnoses require documented provider encounters.
12. Conflicting Documentation Across Records
Discrepancies between progress notes, labs, and discharge summaries create audit failures.
13. Missing Medication or Therapy Documentation
Active treatment without diagnosis linkage weakens medical coding support.
14. Illegible or Scanned Handwritten Records
Poor record quality can invalidate otherwise legitimate diagnoses.
15. Failure to Document Resolved vs. Active Conditions
Historical conditions mistakenly coded as active drive overpayment risk.
Why Do Documentation Gaps Persist Despite Mature Risk Programs?
Even advanced payor organizations struggle with documentation integrity due to systemic provider and operational challenges.
Provider Burden and Time Constraints
Physicians face increasing patient volumes, limiting documentation depth. Studies show documentation quality declines as encounter pressure rises.
Limited Risk Adjustment Education
Many providers are reimbursed fee-for-service, so chronic condition documentation may not be prioritized.
EHR Workflow Fragmentation
Data spread across systems creates incomplete longitudinal records.
Coding–Provider Communication Gaps
Lack of feedback loops prevents documentation improvement.

How Do These Gaps Financially Impact Payor Organizations?
Documentation deficiencies are not administrative nuisances; they are financial liabilities.
- Unsupported diagnoses lead to RADV repayments and penalties
- Expanded CMS audits increase contract-level exposure
- Improper documentation and coding errors cost the industry billions annually
- Coding-related denials surged 126% in recent benchmarking studies
For a mid-sized plan, retrospective review inefficiencies can cost hundreds of millions when extrapolated across populations.
Which Documentation Gaps Trigger the Highest Audit Risk?
While all deficiencies matter, retrospective reviews consistently prioritize high-impact risk areas:
Chronic Condition Validation
Conditions like diabetes, COPD, and CHF require annual re-documentation.
High-RAF Diagnoses
Cancer, ESRD, and transplant status undergo intensified scrutiny.
Sudden Risk Score Spikes
Unusual RAF growth without documentation often triggers audits.
How Are Retrospective Reviews Evolving in 2026 and Beyond?
Audit intensity is accelerating.
- CMS is clearing RADV backlogs and expanding reviews across all contracts
- Retrospective audits now span multiple historical years
- Greater focus is placed on disease specificity and documentation completeness
For leaders, this means retrospective reviews are no longer periodic; they are continuous compliance mechanisms.
What Operational Signals Indicate Documentation Gaps in Your Network?
You can often identify risk before audits begin. Watch for:
- High chart retrieval failure rates
- Low HCC validation scores
- Provider query volumes
- Coding add/delete imbalance
- Denial spikes tied to medical necessity
These signals reflect documentation maturity across your provider ecosystem.
How Can Payor Leaders Close Documentation Gaps at Scale?
Addressing retrospective risk requires a multi-layered strategy.
1. Prospective + Concurrent Reviews
Shift left, don’t rely solely on retrospective correction.
2. Provider Education Programs
Target high-variance providers with audit feedback.
3. Clinical Documentation Improvement (CDI) Alignment
Embed CDI into risk adjustment workflows.
4. Technology-Enabled Chart Mining
AI and NLP accelerate gap detection in large datasets.
5. Two-Way Coding Validation
Add missing diagnoses and delete unsupported ones to ensure audit defensibility.
What Should Leaders Prioritize Now?
If you oversee Risk Adjustment or Provider Network Performance, focus on three executive levers:
Network Documentation Variability
Benchmark providers by validation rate.ft, don’t rely solely on retrospective correction.
Retrospective Review Turnaround Time
Faster reviews reduce extrapolation risk.
Audit Readiness Infrastructure
Ensure that chart retrieval, coding, and compliance teams operate cohesively.
Key Takeaways for Payor Executives
Let’s summarize what matters most for your role:
- Documentation, not coding, drives most audit failures
- Nearly half of coding errors stem from poor documentation
- RADV and commercial audits are expanding in scale and depth
- Chronic condition specificity is now a top validation focus
- Retrospective reviews must evolve into continuous monitoring models
Turning Retrospective Insight into Prospective Advantage
Retrospective reviews are often viewed as compliance exercises. But for forward-thinking payor leaders, they are strategic intelligence tools.
Every documentation gap tells you something:
- Where provider education is lacking
- Which conditions are under-documented
- How RAF accuracy can improve
- Where financial exposure exists
By operationalizing retrospective findings into provider engagement, CDI programs, and analytics-driven monitoring, you move from audit reaction and revenue protection to risk optimization.
And in today’s environment of intensified regulatory scrutiny, that shift isn’t optional, it’s executive-level risk governance.
FAQs
1. What documentation gaps do payors most commonly find during retrospective chart reviews?
Payors most frequently identify missing clinical notes, unsupported diagnoses, lack of MEAT criteria, incomplete chronic condition specificity, unsigned records, and overreliance on problem lists. These gaps directly impact RAF validation and audit defensibility.
2. How do documentation deficiencies affect RAF scores in retrospective risk adjustment reviews?
Incomplete or unsupported documentation leads to diagnosis deletions, lowering validated HCC capture and RAF scores. This can result in revenue loss, repayment risk, and inaccurate population risk stratification.
3. Which diagnoses are most likely to fail validation in retrospective audits?
High-risk chronic conditions such as diabetes with complications, COPD, CHF, vascular disease, cancer, and behavioral health diagnoses often fail when specificity, treatment linkage, or encounter evidence is missing.
4. Why do unsupported diagnoses trigger RADV audit penalties for payors?
CMS RADV audits require medical record evidence proving that diagnoses were monitored, evaluated, assessed, or treated. Unsupported conditions are classified as overpayments, triggering extrapolated financial penalties.
5. How can payors reduce documentation gaps across provider networks?
Payors can implement prospective reviews, provider education, CDI programs, AI-driven chart mining, and coding validation workflows to improve documentation completeness and audit readiness.
6. What is the difference between coding errors and documentation gaps in retrospective reviews?
Coding errors involve incorrect code assignment, while documentation gaps occur when clinical evidence is missing or incomplete. Even correctly coded diagnoses fail audits without sufficient documentation support.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. Led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let’s connect to modernize workflows.