





















One-Sided Risk Is Disappearing: What CMOs Need to Decide Before 2027
The upside-only contract was always a temporary position. CMS structured one-sided risk in MSSP as an on-ramp, not a destination, and it has been narrowing that on-ramp consistently since 2019. The BASIC track glide path toward two-sided risk, and CMS’s stated goal of moving all Medicare beneficiaries into accountable care relationships with downside exposure, make the direction clear. If your ACO or Medicare Advantage contract still operates on a one-sided framework, you are not waiting for change. You are in the middle of it.
The question for CMOs is not whether two-sided risk becomes the norm. It is whether your organization builds the clinical documentation and risk adjustment infrastructure to absorb that risk before the contract terms are written, or after. That sequence matters more than most clinical leaders expect, and the window to influence it is shorter than the contracting calendar suggests.
One-sided risk is already costing you, just not the way you think
The appeal of one-sided risk is structural: shared savings upside with no downside exposure. But the trade-off is built into the benchmark. Under MSSP BASIC tracks, ACOs that avoid downside risk accept a lower savings rate and a benchmark methodology that becomes harder to beat as their quality baseline improves. The longer you operate in upside-only mode, the more your benchmark trends toward your actual cost performance. High performers get rewarded with a tighter corridor.
Medicare Advantage contracts with one-sided structures present a different problem. The payer retains the risk and the margin. When RAF scores are suppressed or HCC capture is incomplete, the organization has no incentive to fix it because there is no cost consequence. That tolerance for undercoding disappears under two-sided risk, and organizations that have not built concurrent documentation programs find out the hard way.
Under two-sided risk, a missed HCC is a direct financial loss
The arithmetic is the same; the consequences are not. When your contract includes downside exposure, every gap between your patient’s actual disease burden and what your documentation supports becomes a line item against your shared loss corridor or capitation budget.
V28 has compounded this. The model reduces the coefficient on certain hierarchical condition categories and removes others from the risk adjustment hierarchy entirely. For organizations whose RAF scores relied on diagnosis categories V28 depresses, the practical effect is a lower per-member capitation rate with the same patient population. That gap has to be recovered through more accurate documentation of the conditions V28 does credit, not by coding the conditions it no longer does.
Retrospective chart reviews cannot bridge this timing gap. Under two-sided risk with a closed performance year, retrospective reviews may not change your actual shared loss exposure for the period already under review. The documentation has to be built before the claim window closes, not after.
Most CDI programs were built for a different problem
CDI programs in most health systems grew up in the inpatient DRG world. The workflows, the query logic, the physician training, and the staffing models were built to improve case mix index on inpatient discharges. That skill set does not translate directly to outpatient HCC capture, which requires ongoing longitudinal documentation of chronic conditions across multiple encounter types.
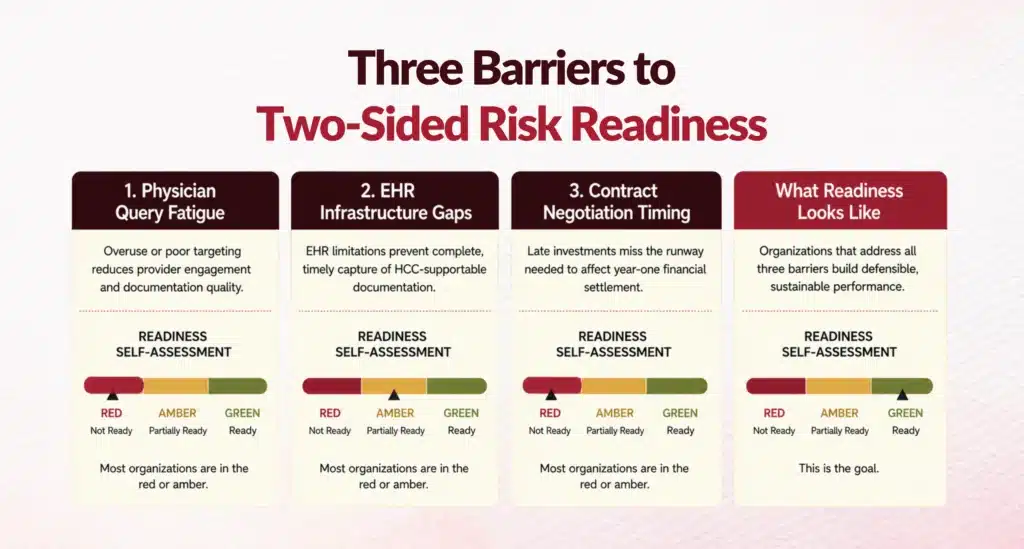
Three structural gaps determine whether an organization holds its RAF position through the transition. Physician query fatigue: when query volume is high and queries feel low-value, response rates fall. Under two-sided risk, a declined query on a high-weight HCC contributes directly to an inaccurate RAF score that your settlement is based on.
EHR infrastructure: many outpatient workflows were not designed to surface chronic condition gaps at the point of care, leaving prospective programs to operate outside the clinical encounter where uptake is limited. Contract negotiation timing: payers evaluate your RAF trajectory, quality scores, and CDI maturity 12 to 18 months before renewal. CMOs who wait until the term sheet arrives are negotiating from a fixed position.
Where does your organization stand on two-sided risk readiness?
Most CMOs entering a contract renewal cycle have a general sense of their risk adjustment position but limited visibility into where the specific gaps are. The difference between a recoverable gap and an exposed one often comes down to whether you identified it before the contract was signed or after the performance year closed.
The Blended-Model Readiness Snapshot is a one-page diagnostic for CMOs and VBC medical directors. It walks through where documentation and RAF gaps typically appear during a one-sided to two-sided transition and identifies the highest-leverage interventions based on contract type, population mix, and CDI maturity.
Download the Blended-Model Readiness Snapshot
The Blended-Model Readiness Snapshot is a one-page diagnostic for CMOs and VBC medical directors. It walks through where those gaps typically appear and identifies the highest-leverage interventions based on contract type, population mix, and CDI maturity.
Download

FAQs
What Is the Difference Between One-Sided and Two-Sided Risk in VBC Contracts?
In a one-sided risk VBC contract, the provider organization shares in savings if costs come in below the benchmark but bears no financial loss if costs exceed it. In a two-sided risk contract, the organization shares in both savings and losses. Under MSSP's current track structure, BASIC track ACOs can enter in upside-only mode but are required to transition toward downside exposure as they accumulate experience. ENHANCED track and most Medicare Advantage capitation arrangements are already two-sided.
How Does the V28 Risk Adjustment Model Affect CMO Contract Strategy?
CMS's V28 update to the HCC risk adjustment model for Medicare Advantage recalibrates the diagnosis categories that carry RAF weight, reducing coefficients on some and removing others from the hierarchy entirely. According to CMS's V28 model documentation, plans and providers whose populations have historically had RAF scores anchored to categories that V28 depresses will see lower capitation rates for the same patients. The strategic response is not to chase the removed categories but to improve documentation accuracy and completeness for the conditions V28 does credit.
When Should a CMO Begin Preparing for a Two-Sided Risk Transition?
The operational answer is 12 to 18 months before your contract renewal date. Documentation programs require physician behavior change, EHR workflow updates, and enough encounter volume to produce measurable RAF improvement. If you start after the contract transitions, you have already absorbed the first performance year under terms that do not reflect your accurate patient acuity. The strategic preparation, including RAF gap analysis and CDI program scoping, should begin well before the contracting cycle opens.
What Does a Concurrent CDI Program Cost vs. What It Recovers Under Two-Sided Risk?
Cost depends on program scope and whether the organization builds internal capacity or partners externally. A concurrent CDI program covering an outpatient Medicare population typically requires dedicated CDI staff, query management tools, and physician training. The recovery depends on the size of your RAF gap. Organizations with meaningful HCC capture gaps relative to their population's actual acuity typically recover multiples of the program cost within the first full contract cycle.
What Happens If an Organization Does Not Address Documentation Gaps Before a Two-Sided Contract Starts?
The most direct consequence is a RAF score that understates your patient population's disease burden during the first performance year under two-sided risk. Because capitation rates and shared loss calculations are both based on risk-adjusted benchmarks, an understated RAF translates into a lower revenue ceiling and a shared loss exposure that is calculated against a cost performance figure that does not account for your patients' actual acuity. Fixing that gap retrospectively after the performance year closes may not change your settlement for that period.
How Do CMOs Use Contract Negotiation Timing as a Strategic Lever?
Payers and CMS evaluate provider organizations on their RAF trajectory, quality score trends, and CDI program maturity when setting contract terms. CMOs who can present auditable documentation of their HCC capture rate improvement, their CDI infrastructure, and their physician query management performance enter renewal negotiations with evidence that reduces the payer's perceived downside risk. That evidence base directly affects the corridor structure, the savings rate, and the benchmark methodology offered in the new contract. Organizations without it negotiate from assumptions, not data.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. I've led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let's connect to modernize workflows.