


















Concurrent Coding vs Retrospective Audits: A Side-by-Side Revenue Comparison
Why Back-End Audits Alone Can’t Safeguard Modern Healthcare Revenue?
Healthcare revenue integrity is no longer protected at the back end. If you lead CDI, HIM, or Revenue Cycle, you already know the reality: waiting until discharge to identify documentation and coding gaps is financially reactive, not strategic.
Here’s the direct answer to the primary question:
Concurrent coding consistently delivers higher net revenue capture, lower denial rates, faster case mix index (CMI) lift, and reduced audit risk compared to retrospective audits, because it corrects documentation in real time, before claims are finalized.
Retrospective audits still have value for compliance and trend analysis, but they recover only what remains fixable after discharge. In today’s audit-heavy, margin-compressed environment, that gap directly translates into lost reimbursement.
Let’s break this down side by side.
What Is the Core Difference Between Concurrent Coding and Retrospective Audits?
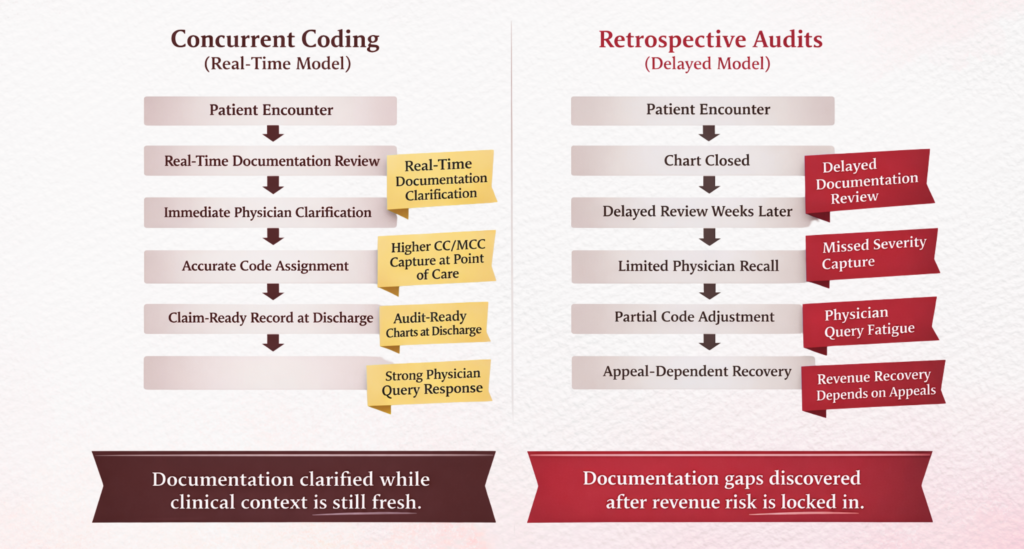
Concurrent Coding - Revenue Protection in Real Time
Concurrent coding occurs while the patient is still admitted. CDI specialists and coders review documentation simultaneously, querying providers before discharge.
This enables:
- Real-time diagnosis clarification
- Severity of illness (SOI) accuracy
- Risk of mortality (ROM) capture
- DRG optimization before billing
Because documentation is still editable, financial impact is immediate.
Retrospective Audits - Revenue Recovery After the Fact
Retrospective reviews happen post-discharge, often weeks or months later.
Their purpose is to:
- Validate coding accuracy
- Identify missed diagnoses
- Ensure compliance
- Prepare for external audits
However, once the claim is billed, correction pathways narrow, often requiring rebilling, appeals, or write-offs.
How Does Revenue Impact Compare Side by Side?
Let’s talk about financial outcomes, the metric your CFO cares about most.
Case Mix Index (CMI) Lift
Industry benchmarks from CDI programs reported through organizations like AHIMA and ACDIS show:
- Concurrent CDI programs can drive CMI increases of 3%–7% within the first year.
- Retrospective audits typically yield 1%–2% retrospective recovery.
Why the difference?
Because concurrent coding captures:
- MCCs/CCs in real time
- Hierarchical Condition Categories (HCCs)
- Procedure specificity
Once discharged, many of these cannot be added compliantly.
Revenue per Case
HFMA revenue integrity analyses indicate:
- Concurrent review programs can improve revenue per case by $1,500–$3,000 in high-acuity service lines.
- Retrospective audits recover smaller amounts, often $300–$900 per case, due to documentation finality.
For a 250-bed hospital, that difference can translate into $3M–$7M annual variance.
Which Model Reduces Denials More Effectively?
Denial prevention is where concurrent coding dominates.
Concurrent Coding Denial Impact
Real-time documentation alignment ensures:
- Medical necessity support
- DRG validation accuracy
- Procedure justification
- Length-of-stay alignment
CMS and OIG audit findings consistently show that documentation insufficiency is a leading cause of payment denials and RADV extrapolations.
By addressing gaps pre-bill, concurrent coding reduces:
- Clinical validation denials
- DRG downgrades
- Medical necessity denials
Many health systems report 10%–20% denial reduction after implementing concurrent CDI reviews.
Retrospective Audit Denial Impact
Retrospective audits:
- Identify denial root causes
- Support appeal writing
- Inform education
But they do not prevent the initial denial.
Appeal success rates vary widely, often landing between 35%–55%, according to payer dispute benchmarking studies.
That means nearly half of the identified revenue is never recovered.
How Do Both Models Perform Under External Audit Scrutiny?
Audit exposure is rising rapidly, especially with CMS expanding RADV and Targeted Probe and Educate (TPE) reviews.
Concurrent Coding and Audit Defense
Concurrent documentation strengthening improves:
- Diagnosis clinical validation
- Physician attribution clarity
- Treatment linkage
- Problem list accuracy
This creates audit-ready charts at discharge.
CMS emphasizes documentation integrity as the foundation of compliant reimbursement.
Hospitals with mature concurrent CDI programs often demonstrate:
- Lower extrapolated audit penalties
- Faster audit response times
- Reduced payer recoupments
Retrospective Audits and Compliance Risk
Retrospective reviews are essential for:
- Identifying systemic coding risk
- Monitoring coder accuracy
- Preparing for RAC/MAC audits
But they operate after exposure already exists.
If unsupported diagnoses were billed, repayment risk remains, even if caught internally later.
What Are the Operational Cost Differences?
Leaders often ask: Does concurrent coding cost more to run?
Short answer: Yes operationally, but not financially.
Concurrent Coding Investment Areas
You’ll need:
- CDI specialists
- Physician query workflows
- EHR integration tools
- Real-time coding resources
Upfront labor costs are higher.
However, ROI analyses from revenue integrity programs show:
- 3:1 to 7:1 return ratios
- Break-even timelines under 12 months
This is driven by sustained CMI lift and denial avoidance.
Retrospective Audit Cost Profile
Retrospective reviews cost less to operate because they require:
- Smaller teams
- No real-time provider engagement
- Batch review workflows
But revenue yield is also lower.
They function more as compliance insurance than revenue growth engines.
How Does Physician Engagement Differ?
Physician alignment is a major success factor.
Concurrent Coding Physician Impact
Concurrent workflows enable:
- Immediate clarification queries
- Documentation education in context
- Behavioral reinforcement
Studies published in CDI practice journals show providers are more responsive to queries during active care vs. post-discharge.
It feels clinically relevant, not administrative.
Retrospective Audit Physician Impact
Post-discharge queries face:
- Recall gaps
- Lower response rates
- Documentation addendum resistance
This limits financial correction potential and slows rebilling timelines.
Which Model Better Supports Value-Based Care and Risk Adjustment?
As reimbursement shifts toward risk models, documentation timing becomes critical.
Concurrent Coding in Risk Models
Concurrent reviews strengthen:
- HCC capture
- RAF accuracy
- Chronic condition specificity
- Quality measure alignment
This directly impacts:
- Medicare Advantage reimbursement
- Bundled payment performance
- Shared savings outcomes
Accurate capture must occur before claim submission to influence actuarial calculations.
Retrospective Reviews in Risk Models
Retrospective audits help:
- Identify missed HCC trends
- Educate providers
- Refine future documentation
But they rarely affect the already-submitted risk period.
When Should Organizations Use Both Models Together?
This isn’t an either-or decision for most mature health systems.
Best practice revenue integrity frameworks deploy both:
Concurrent Coding for:
- Real-time revenue capture
- Denial prevention
- CMI optimization
- Audit readiness
Retrospective Audits for:
- Compliance monitoring
- Coding accuracy validation
- Education planning
- External audit preparation
Think of concurrent coding as revenue offense and retrospective audits as compliance defense.
You need both, but one drives financial growth.
What Does the Future Revenue Model Look Like?
AI-enabled concurrent coding is accelerating adoption.
Advanced platforms now support:
- Real-time NLP diagnosis detection
- Auto-query prioritization
- Clinical validation alerts
- DRG drift monitoring
CMS continued audit expansion and payer pre-payment review growth make retrospective-only models financially risky.
Revenue leaders are shifting left, embedding documentation integrity at the point of care.
The Bottom Line - Which Model Wins Financially?
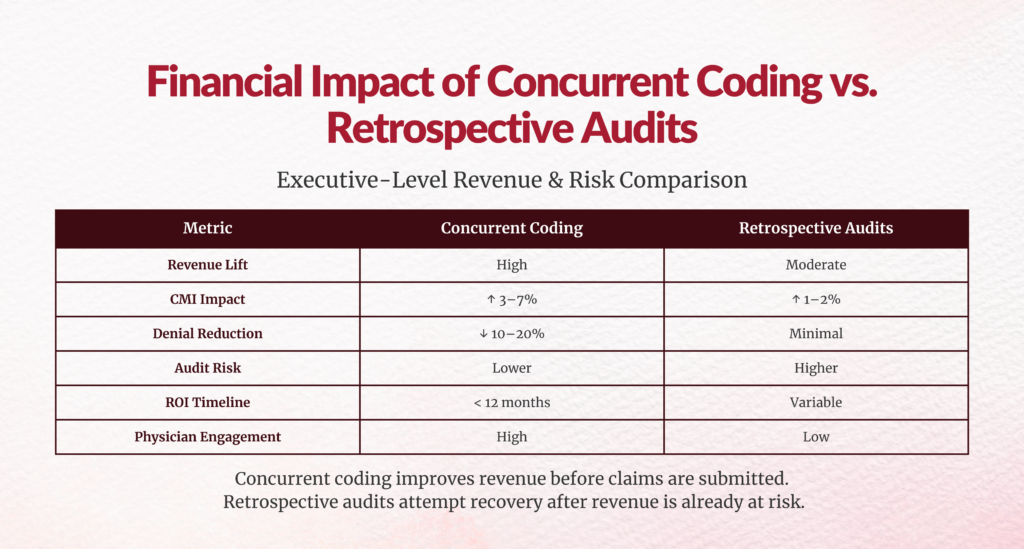
| Metric | Concurrent Coding | Retrospective Audits |
|---|---|---|
| Revenue Lift | High | Moderate |
| CMI Impact | 3%–7% | 1%–2% |
| Denial Reduction | Significant | Minimal |
| Audit Readiness | Strong | Reactive |
| Physician Engagement | High | Low |
| Compliance Monitoring | Moderate | Strong |
| ROI Timeline | <12 months | Variable |
Final Thoughts for Leaders
If you’re responsible for margin protection, here’s the strategic takeaway:
- Retrospective audits tell you what you missed.
- Concurrent coding ensures you don’t miss it in the first place.
In an environment shaped by RADV expansion, payer scrutiny, and value-based reimbursement, revenue integrity must begin before discharge, not after billing.
For CDI Directors, HIM leaders, and CFOs alike, the financial math is clear:
Real-time documentation integrity is no longer optional, it’s foundational to sustainable reimbursement.
FAQs
1. What is the revenue difference between concurrent coding and retrospective audits?
Concurrent coding typically delivers higher financial impact because documentation gaps are corrected in real time. Industry benchmarks show concurrent CDI programs can drive 3%–7% case mix index (CMI) improvement, while retrospective audits usually recover only 1%–2% in missed revenue after discharge.
2. Does concurrent coding reduce claim denials compared to retrospective reviews?
Yes. Concurrent coding reduces denials more effectively because medical necessity, severity, and diagnosis documentation are validated before claims are submitted. This prevents clinical validation and DRG downgrade denials that retrospective audits can only address after they occur.
3. Is retrospective auditing still necessary if we implement concurrent coding?
Absolutely. Retrospective audits remain critical for compliance monitoring, coding accuracy validation, and audit preparedness. Best-practice revenue integrity models use concurrent coding for real-time revenue capture and retrospective audits for risk surveillance and education.
4. How does concurrent coding impact case mix index (CMI) growth?
Concurrent coding improves CMI by ensuring CCs, MCCs, and severity indicators are documented before discharge. Real-time physician queries strengthen SOI and ROM capture, leading to sustained reimbursement increases across inpatient populations.
5. Which model is more effective for audit readiness and RADV scrutiny?
Concurrent coding provides stronger audit defense because documentation is validated at the point of care. This reduces unsupported diagnoses and repayment risk during CMS or payer audits. Retrospective audits help identify risks but occur after exposure already exists.
6. What ROI can hospitals expect from concurrent coding programs?
Most organizations see ROI within 12 months. Revenue gains from CMI lift, denial reduction, and documentation accuracy often produce 3:1 to 7:1 returns, making concurrent coding a high-impact revenue integrity investment.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. Led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let’s connect to modernize workflows.