





6 Steps to Prepare for the CMS HCC Model V28 – 2026
Understanding the 2026 V28 Cliff
In 2026, the Centers for Medicare & Medicaid Services (CMS) will finalize the three-year transition to the V28 risk adjustment model, ending the era of blended V24/V28 scoring. For Payment Year (PY) 2026, 100% of RAF scoring will be based on V28, meaning V24 codes will disappear overnight from reimbursement calculations.
According to CMS projections, organizations that do not re-align documentation and coding could face a 5–15% decline in RAF scores, directly impacting reimbursement and financial stability.
In simple terms, if your organization is still using “transition mode,” 2026 will be a revenue cliff.
This blog breaks down six actionable steps healthcare leaders, HIM Directors, Revenue Cycle Directors, VP of Rev Cycle, and RCM executives must take now to protect revenue and ensure compliance under V28.
What Makes V28 So Different from V24?
Before preparing your organization, you need to understand the magnitude of the shift.
| Feature | V24 (Legacy) | V28 (2026 Full Implementation) | Impact |
|---|---|---|---|
| Phase-In Status | 33% of the score (in 2025) | 100% of score (in 2026) | V24 codes eliminated |
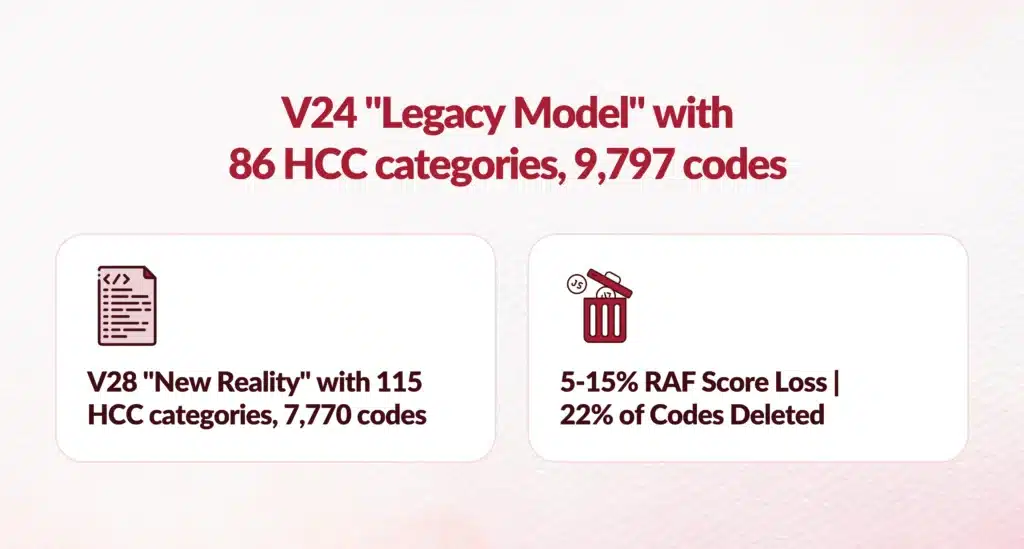
| HCC Categories | 86 | 115 | Higher granularity |
| Diagnosis Codes | ~9,797 | ~7,770 | 2,000+ codes deleted |
| Code Logic | ICD-9 legacy | ICD-10 specificity | Severity becomes essential |
| Example | PVD coded & risk-adjusted | PVD removed, only Atherosclerosis w/ ulcer/gangrene maps | Unspecified = Zero Value |
Statistic: Nearly 22% of current RAF scores rely on codes that will have no value in V28.
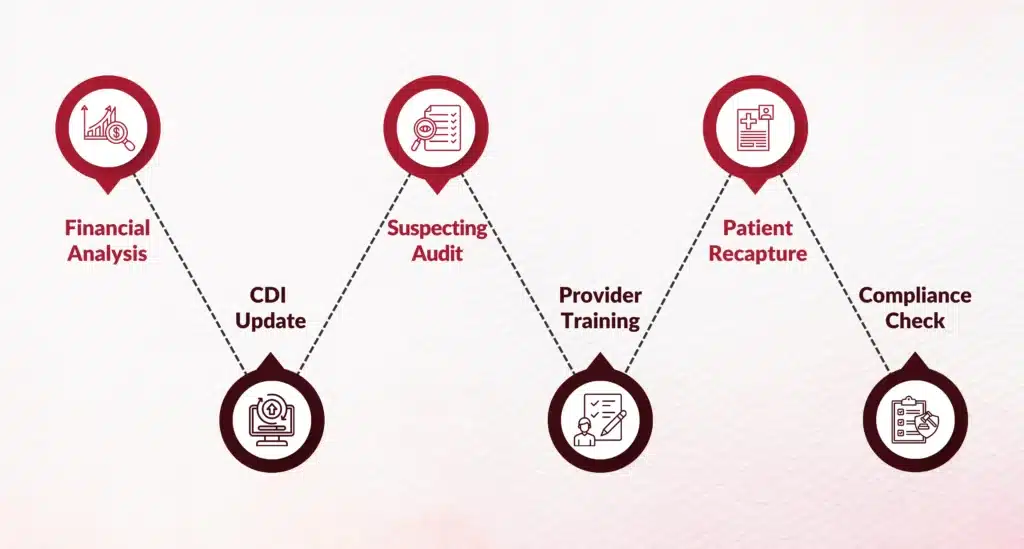
How Can Healthcare Organizations Prepare?
Below are the six steps you must implement before Q1 2026 to ensure financial stability and compliance.
Step 1: How Do You Perform a V28-Only Financial Impact Analysis?
Most organizations still evaluate blended RAF performance, masking the real exposure to revenue loss.
Action
Run a shadow RAF assessment using 100% V28 logic, across service lines, provider groups, and chronic patient cohorts.
Goal
Identify “V24-dependent” populations, patients whose risk scores depend on codes like:
- I73.9 — Peripheral Vascular Disease
- I20.9 — Angina Pectoris
Insight
Organizations that conduct V28-only forecasting early in 2025 are 3× more likely to meet PY2026 revenue targets.
Step 2: How Should CDI Teams Adapt for V28 Documentation Specificity?
In V28, “unspecified” = “unrecognized.” If the diagnosis lacks severity or complication details, it does not risk-adjust.
The New Rule
“If it isn’t clinically specific, it likely won’t count.”
Code This - Not That (V28 Examples)
| Condition | Avoid This | Use This Instead |
|---|---|---|
| Depression | F32.0 (removed) | F32.A / F33.2 (severity needed) |
| PVD | I73.9 (deleted) | I70.235 (with ulcer/gangrene) |
| Angina | I20.9 (removed) | I20.0 (unstable) |
Best Practice
HIM & CDI teams must shift from diagnosis capture to severity documentation with templates and prompts built directly into the EHR.

V28 Transition: Revenue Protection & Compliance Strategy
Step 3: Is Your Suspecting Logic Still Recommending V24 Codes?
Many suspecting engines still surface obsolete V24 codes, distracting providers and reducing encounter quality.
Actions
- Audit suspecting logic immediately
- Remove non-risk-adjustable V24 alerts
- Rebuild indicators for chronic complications, not symptoms
EHR Example
Instead of “Suspect Diabetes,” recommend:
“Suspect Diabetes WITH neuropathy or CKD, review chart for complications.”
Result
Reduced alert fatigue. Higher coding precision. Lower provider frustration.
Step 4: What’s the Best Way to Train Providers on V28?
Traditional coding training won’t work. You must teach WHY the clinical documentation changes, not just what to code.
Training Strategy
- Host specialty-specific briefings
- Show “Top 5 Deleted Codes” per specialty
- Explain how severity affects risk
Example: Diabetes Under V28
In V28, “with acute complications” and “without complications” carry nearly the same RAF value.
Only chronic complications (neuropathy, nephropathy, retinopathy) drive value.
Teach clinicians: “Don’t just capture the problem, capture its clinical consequence.”
Step 5: How Should You Recapture & Re-Evaluate Patients?
Patients whose only qualifying HCC is being deleted in V28 will vanish from your risk registry in 2026.
Action Plan
- Identify patients who will drop off the risk list
- Schedule re-evaluation & follow-up visits
- Determine if more clinically accurate conditions exist
Example
A patient previously coded with:
Major Depressive Disorder, Unspecified (F32.9)
may actually have:
Major Depression, Moderate (F32.1) to V28-compliant & valid
Objective
Recapture only legitimate risk, backed by clinical evidence.

Step 6: How Do You Prevent “Severity Creep” and Compliance Risks?
As revenue declines, organizations may feel pressured to increase severity coding, a red flag for CMS audits.
Why This Matters
OIG has already stated that V28-related severity upcoding will be monitored closely.
Defense Strategy
- Pre-bill audits for high-risk HCCs
- Require lab values or treatment plans to justify severity
- Track sudden shifts in diagnosis patterns
Compliance Rule
Every severe diagnosis must be defensible. If CMS requests proof, can your team produce it instantly?
What’s the Best Timeline to Follow Before V28 Goes Live?
| Timeline | Required Actions |
|---|---|
| Q1–Q2 2025 | 100% V28 financial impact assessment + IT suspecting audit |
| Q3–Q4 2025 | Provider education + documentation specificity training |
| Jan 1, 2026 | All claims must follow V28 coding requirements |
What Should Leaders Do Right Now?
If you wait until 2026, you will be too late.
Your immediate priorities should be:
- Run V28-only RAF analytics
- Audit CDI documentation & suspecting logic
- Launch targeted provider education
- Establish compliance guardrails
Healthcare leaders who move now will protect revenue, reduce compliance risk, and transition successfully into V28 without disruption.
Need Help Implementing V28?
If you need a V28 financial impact audit, provider documentation training, or suspecting algorithm updates, we can guide your organization through every phase of implementation.
Let’s ensure your organization doesn’t fall off the 2026 cliff, but leads from ahead.
FAQs
What is the CMS HCC Model v28 and when does it take effect?
CMS-HCC Model v28 fully takes effect January 1, 2026 for Payment Year 2026, ending V24/V28 blended scoring; expands to 115 HCCs from 86 with refined ICD-10 mappings emphasizing clinical severity.
Why are RAF scores expected to drop under the v28 model?
V28 eliminates 2,294 V24 diagnosis codes, reduces from 9,797 to 7,770 mappings, prioritizes severity over volume, creating V24-dependent revenue cliffs for chronic cohorts.
How will HCC v28 changes affect provider reimbursement?
100% V28 RAF calculation removes legacy codes overnight, potentially lowering scores 10-20% for V24-reliant providers unless documentation shifts to severity specificity.
What documentation practices improve HCC capture before 2026?
Shift to severity documentation (nephropathy, neuropathy vs. generic diabetes), EHR templates/prompts, MEAT criteria strengthening, suspecting logic V28 alignment.
What six steps should organizations take now to prepare for v28?
1. V28-only financial impact analysis; 2. Audit suspecting tools; 3. Provider education; 4. Documentation templates; 5. Analytics dashboards; 6. Q1-Q4 2025 timeline execution.
How does provider education support risk mitigation for HCC changes?
Trains on V28 hierarchies/complications, reduces alert fatigue with precise suspecting, improves coding precision, meets 3x higher revenue target likelihood.
What analytics methods help forecast RAF score impact?
Shadow RAF assessments (100% V28 logic), service line/provider cohort analysis, V24-dependent population modeling, query compliance tracking.
How should CDI and risk teams align for HCC readiness?
Joint V28 mapping reviews, shared dashboards, concurrent validation, severity-focused querying, cross-training on clinical/coding hierarchies.
What role do clinical data quality and structured documentation play in HCC accuracy?
Ensures MEAT compliance, definitive diagnoses, hierarchy adherence; V28 demands stronger clinical indicators vs. V24 volume coding.
How are payers responding to CMS Model v28 changes?
MA plans accelerate V28 readiness, audit historical coding, deploy AI CDI/CAPD tools, monitor provider RAF shifts for compliance/risk.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. Led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let’s connect to modernize workflows.