





















417 Rural Hospitals Are Facing a New Financial Crisis
Why 417 Rural Hospitals Are Facing a New Financial Crisis and What It Means for Healthcare Access?
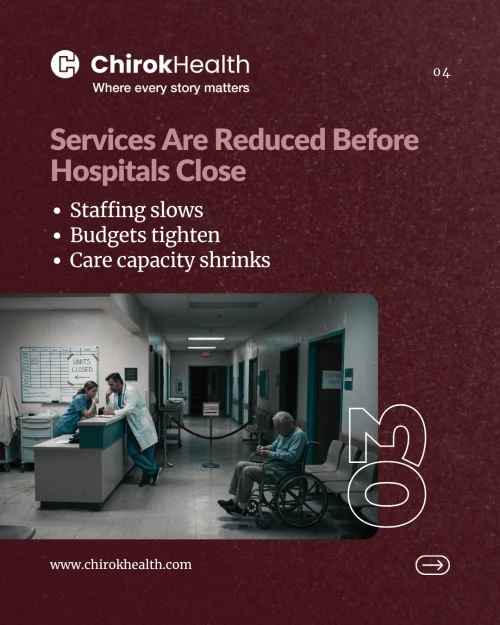
It’s becoming increasingly difficult to sustain healthcare operations in an environment where costs are rising, reimbursements are tightening, and patient volumes remain unpredictable, especially for rural providers.
At best, this results in already thin operating margins becoming even slimmer. At worst, it puts hospitals on a path toward service reductions, conversion, or complete closure.
A recent report from Chartis highlights the severity of the situation: 417 rural hospitals across the United States are currently vulnerable to closure.
As per Chartis’ Rural Hospital Vulnerability Index report, which evaluates multiple operational, financial, and market-based indicators to assess hospital closure risk.
“Dozens of rural hospitals are already at risk of closure, and without meaningful policy support, that number will only grow.”
The State-Level Reality of Rural Healthcare Is Shifting
Although the overall number of vulnerable rural hospitals has slightly declined, state-level data reveals a more concerning and uneven reality across rural healthcare systems.
Some states are seeing increased vulnerability, with rural hospitals at risk:
Tennessee: 44% to 61%
South Dakota: 28% to 42%
Others have shown modest improvement:
Mississippi: 49% to 42%
Kansas: 47% to 44%
In total, 17 states now have at least 10 rural hospitals at risk of closure. Leading the list are
Texas (50 hospitals)
Kansas (44)
Tennessee (27)
Georgia (25)
Mississippi (24)
These states are also among those receiving a combined $1.1 billion in funding through the Centers for Medicare & Medicaid Services Rural Health Transformation initiative, highlighting both the scale of the challenge and the urgency to stabilize rural healthcare access.
“There’s no guarantee that critical funding will reach rural hospitals, and that uncertainty puts their future at risk.”
When Rural Care Delivery Becomes Unsustainable?
Since 2010, 206 rural hospitals have either closed or transitioned away from inpatient care to alternative care models, as reported by Becker’s Hospital Review.
“Rural hospitals don’t control the factors that determine their survival, funding decisions are often made far beyond our walls.”
Brian Sponseller, CEO, Carolina Pines Regional Medical Center
In many cases, hospitals are not shutting down entirely but are instead shifting to a newer model, the Rural Emergency Hospital (REH) designation. This allows facilities to continue offering emergency and outpatient services while eliminating inpatient care.
As of early 2026, 44 hospitals across 18 states have made this transition.
Some examples include
- Bullock County Hospital (Alabama)
- Sturgis Hospital (Michigan)
- Clifton Fine Hospital (New York)
- Irwin County Hospital (Georgia), and
- Falls Community Hospital and Clinic (Texas)
This shift reflects a difficult but necessary decision within rural healthcare: maintaining some level of care access rather than losing services entirely.

How Long Can Rural Healthcare Systems Operate Under Pressure?
For many rural hospitals, financial strain is not temporary, it is structural. While healthcare systems may experience periodic fluctuations, persistent negative operating margins signal a deeper challenge within rural healthcare economics.
When losses become the norm rather than the exception, sustainability becomes increasingly difficult.
Hospital leaders are often caught between two competing priorities:
Maintaining rural healthcare access in underserved communities
Ensuring the financial health of their organization
Balancing these demands is complex, and in many cases, there is no clear or easy solution.
Top Reasons Behind Rural Hospital Closures
- Rising Operating Costs and Inflationary Pressures
Labor shortages, wage inflation, and supply chain challenges continue to increase the cost of care delivery.
Unlike large health systems, rural hospitals cannot negotiate better vendor rates, and spread costs across high patient volumes. This results in higher cost per patient and lower margins per service.
- Declining Reimbursements and Unfavorable Payer Mix
Rural hospitals serve a higher proportion of Medicare patients and Medicaid beneficiaries. These programs typically reimburse at lower rates than commercial insurance.
At the same time, even private insurers are not consistently covering the full cost of care.
“Rural hospitals are fighting every day for fair reimbursement, it’s a constant battle just to stay viable.”
Randall Dauby – CEO, Pinckneyville Community Hospital
- Healthcare Staffing Shortages and Workforce Challenge
Recruiting and retaining clinical staff in rural areas remains difficult. Hospitals are often forced to pay premium wages and rely on temporary staffing. Both of which increase operational costs without increasing revenue.
- The Financial Impact of Low Payments from Private Insurers
A less discussed, but critical, issue is that private insurers often reimburse rural hospitals at lower rates than expected. In some cases, payments are lower than Medicare, nearly 40%–50% of hospital services are impacted.
The Impact of Hospital Closures on Rural Populations
Behind every statistic is a rural community that depends on its hospital, not just for emergency services, but for ongoing care, employment, and economic stability.
When a rural hospital closes or reduces services:
Longer travel for care:
When there’s no local hospital, even a routine checkup means a long drive. If there’s an emergency? That distance feels endless, and honestly, it’s frightening for families.
Slower emergency response:
Ambulances have to cover more ground now. Every extra mile adds crucial minutes, and waiting for help feels agonizing.
Loss of preventive care:
Without a hospital nearby, getting regular checkups or managing chronic problems gets tough. Issues that a simple screening could catch early can slip through the cracks and become real trouble.
Mental health strain:
Hospitals often anchor behavioral health services, too. When those close, people who count on therapy or counseling are left out in the cold, scrambling for support that might not even exist.
Vulnerable populations:
Seniors, families without a lot of resources, folks who can’t just jump in a car, these are the people who suffer most. For them, getting to a doctor sometimes just isn’t possible.
Disrupted continuity of care:
Losing your hospital means losing the doctors and nurses you know and trust. Patients end up confused, treatment plans fall apart, and stress balloons for everyone involved.
Strain on nearby hospitals:
The pressure shifts to the next closest facility. Suddenly, it’s packed. Staff burn out, wait times climb, and giving every patient proper attention gets a lot harder.
Community health decline:
Fewer options for care drag everyone down. Chronic problems get worse, preventable diseases spread, and the whole community’s well-being takes a hit.
These are real consequences that extend far beyond financial performance, reinforcing that rural healthcare challenges are as much about communities as they are about numbers.
Understanding the Financial Pressures Facing Rural Hospitals
If you spend any time talking to leaders in rural healthcare, one thing becomes clear pretty quickly, there isn’t a single issue causing the strain we’re seeing today.
It’s not just costs, staffing, and patient volumes. It’s all of it, happening at the same time, and interacting in ways that make the situation harder to manage than it might appear on the surface.
The rising hospital cost, and workforce shortages are real. The volumes in many areas are lower than what hospitals need to stay financially healthy.
But what often gets missed is something more fundamental:
how consistently hospitals are able to turn the care they provide into actual, realized revenue.
Because in many cases, the care is being delivered. The need is there. But the financial return doesn’t fully reflect that reality. Over time, that gap starts to matter a lot.
From what we’re seeing, there are a couple of signals that tend to show up when that gap becomes too big to ignore.
Key Risk Indicators of Financial Vulnerability
Sustained Negative Margins
Most hospitals can absorb a tough year. Sometimes even two. That’s part of operating in healthcare.
But when losses stretch across multiple years, it usually means something deeper is off.
And it’s not always as simple as “costs are too high.” More often, it’s a combination of things that don’t quite line up:
- Services that aren’t fully captured in billing
- Clinical complexity that doesn’t translate cleanly into reimbursement
- Payments that take too long, or never fully materialize
None of these issues, on their own, seem catastrophic. But they don’t happen in isolation.
They build on each other. Quietly at first. Then all at once. And in rural settings, where margins are already tight, there’s very little room to absorb that kind of accumulation.
Dependence on Medicaid Reimbursement
Rural hospitals are often the primary access point for Medicaid patients. That’s not just part of their role, it’s central to it.
But it also creates a tough financial dynamic. Reimbursement levels are lower. That’s the reality.
Which means hospitals have less flexibility to navigate inefficiencies or absorb missed revenue. So the margin for error shrinks.
In that kind of environment, details matter more. If documentation is incomplete, if coding isn’t precise, if billing isn’t tight, the financial impact shows up quickly. And it’s not always easy to recover from.
Where Financial Pressures Surface in Hospital Operations?
These challenges aren’t theoretical. They show up in very practical ways across hospital operations.
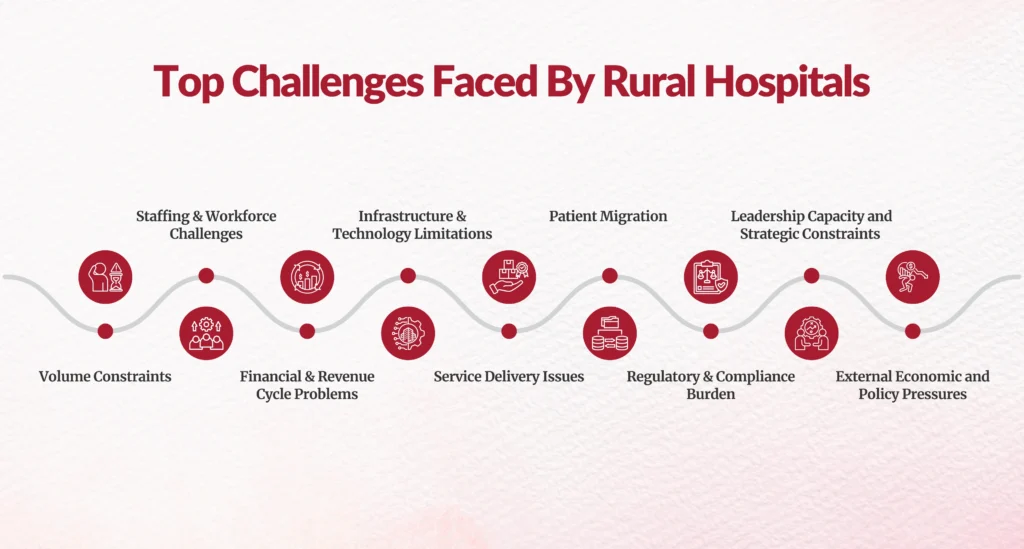
Volume Constraints and Fixed Cost Structures
Rural hospitals don’t have the benefit of high patient volumes. That’s just part of the landscape.
But cost reduction doesn’t happen in the same way. So every patient encounter carries more weight. Not just clinically, but financially.
There isn’t much room to “make it up later.” If revenue is delayed or missed, it’s felt almost immediately.
Workforce Challenges Across Clinical and Operational Teams
When we talk about staffing, the focus is usually on clinicians, and rightly so.
But there’s another side to it. Teams handling documentation, coding, billing, and follow-up are often just as stretched. Sometimes more.
And when those teams are under pressure, things slow down:
- Claims take longer to go out
- Errors become more likely
- Follow-ups get delayed
It doesn’t take much for that to start affecting cash flow.
Increasing Complexity in Payment and Reimbursement
Even when everything is done right on the clinical side, payment isn’t guaranteed, or at least not timely.
- Denials are more common.
- Payer requirements are more complex.
- Reimbursement timelines are longer.
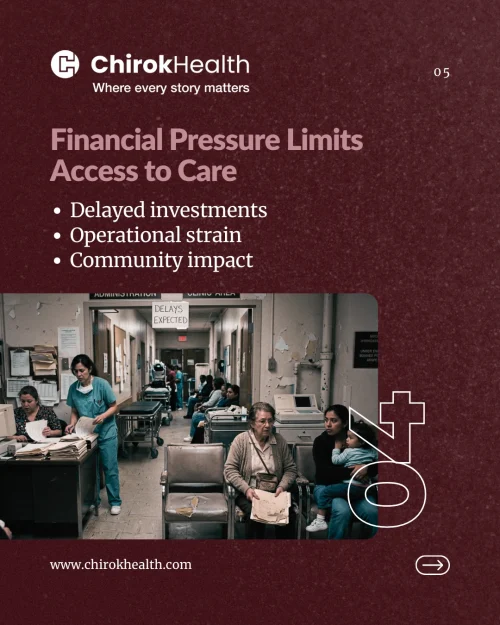
For hospitals with limited reserves, that lag creates real stress. It’s not just an accounting issue, it affects day-to-day operations.
Technology and Infrastructure Limitations
There’s a lot of conversation around using technology to improve efficiency, and that’s valid. But the reality is, many rural hospitals don’t have access to fully integrated systems or advanced tools.
Instead, they’re working with:
Limited automation
Systems that don’t always talk to each other
Gaps in visibility when it comes to performance data
And without clear visibility, it’s hard to fix problems early. Most teams end up reacting instead of getting ahead of issues.
Service Line and Care Delivery Trade-offs
At a certain point, financial pressure forces difficult decisions.
Hospitals start asking:
Which services can we realistically sustain?
Where do we need to scale back?
How do we keep core services intact?
That can mean reducing specialties, consolidating departments, or shifting more toward outpatient care.
“We’re being forced to make difficult decisions,like cutting unprofitable services, just to keep our doors open.”
Rick Smith – CEO, Troy Regional Medical Center
But even those decisions don’t always solve the underlying issue, especially if reimbursement still doesn’t align with the care being delivered.
Market Competition and Patient Migration
Larger systems have advantages, more services, more resources, more visibility. Patients notice that.
And over time, some begin seeking care outside their local communities. Not always, but enough to make a difference.
For rural hospitals, even small shifts in volume can have a meaningful financial impact.
Regulatory and Compliance Burden
Regulatory requirements aren’t new, but they are becoming more complex. For smaller hospitals, keeping up takes time and effort that’s already in short supply.
And when something slips, whether it’s a delay, an error, or a compliance gap, there can be financial consequences tied to it.
Leadership Capacity and Strategic Constraints
Most rural hospital leadership teams are doing a lot with very little. The priority is clear: keep services running, support staff, take care of patients.
But that often leaves limited time for longer-term work, things like operational redesign, financial optimization, or strategic planning.
Not because they’re not important. But because there are only so many hours in the day.
Community Health and Socioeconomic Factors
Rural hospitals don’t operate in a vacuum. The communities they serve often face:
- Higher chronic disease burden
- Transportation challenges
- Financial constraints
All of that affects how patients access care, and whether payments are ultimately collected. It adds another layer to an already complex situation.
External Economic and Policy Pressures
On top of everything else, hospitals are navigating broader changes, economic shifts, policy updates, evolving care models.
These aren’t things they can control. But they still have to respond to them. Often without additional resources.
Bringing It All Together: A Convergence of Financial Pressures
What makes this especially difficult isn’t any one of these challenges on its own. It’s how they stack up.
- Low volume meets fixed costs.
- Operational gaps create the need to optimize reimbursement.
- Limited resources meet increasing complexity.
Over time, it creates a kind of compounding effect. And that’s where stability starts to feel out of reach.
The Path Forward for Rural Hospital Sustainability
Understanding these dynamics is essential, not just to explain the current state, but to inform what comes next.
While the rural hospital financial challenges are significant, there are still opportunities to improve performance:
Because even in this environment, there are opportunities,
to tighten processes, improve documentation, reduce leakage, and make operations more consistent.
And in rural healthcare, small improvements, done well and done consistently, can make a real difference.
What Needs to Change to Prevent Further Rural Hospital Closures?
There isn’t a single fix for the challenges rural hospitals are facing today.
The problem runs deeper than any one issue, it’s systemic. And because of that, the solution has to be just as comprehensive.
Real progress will only happen when policy, operations, and financial strategy start working together, not in silos.
At the core, three things need attention:
First, reimbursement needs to reflect reality.
Rural hospitals don’t operate at high volumes, but they still carry significant fixed costs. Payment models often fail to account for this imbalance, making it difficult for these hospitals to stay afloat.
Second, operations have to become more efficient.
That doesn’t mean cutting corners on care. It means reducing unnecessary administrative work, improving workflows, and making better use of limited resources.
Third, revenue needs to be more predictable.
Hospitals can’t plan for the future if their income is uncertain. Stability and transparency in revenue streams are essential for long-term decision-making.
“Sustaining a rural hospital today requires finding entirely new revenue streams – it’s no longer optional.”
But beyond these structural changes, there’s also a mindset shift that needs to happen.
Rural hospitals are often judged using the same benchmarks as large, urban health systems. That comparison doesn’t hold up. Rural healthcare operates under very different conditions, and until that’s fully recognized, it will be hard to design solutions that actually work.
Improving Financial Stability: What Can Be Done Now
The challenges are real but that doesn’t mean there aren’t ways forward.
Even within today’s limitations, rural hospitals have opportunities to strengthen their financial footing.
Strengthening Financial Performance Through Revenue Cycle Optimization
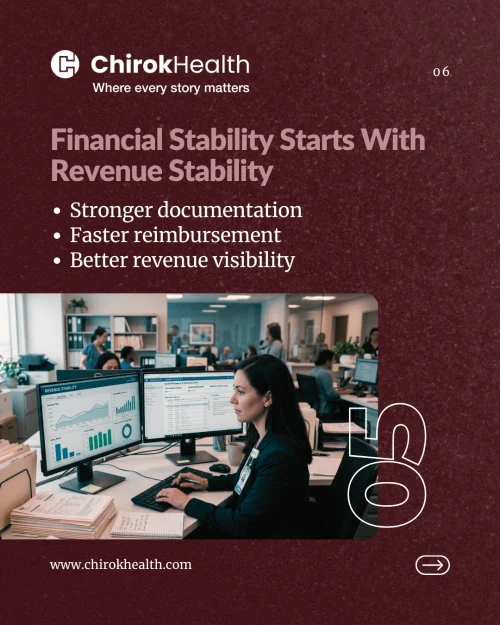
When billing is accurate and processes are efficient, the impact is immediate, reduced claim denials, and cash flow becomes more predictable. In a low-margin environment, even small improvements can go a long way.
The revenue cycle optimization can lead to faster claim submissions, fewer errors in billing and reduced back-and-forth with payers
When processes are streamlined and consistent, claims move more efficiently through the system. This reduces delays, minimizes rework, and ultimately improves cash flow.
Improving Clinical Documentation to Reflect True Patient Complexity
When patient complexity is clearly and fully captured, coding becomes more accurate, and reimbursement better reflects the care being delivered. It also supports better quality reporting and smoother coordination across care teams.
Strengthening documentation practices helps ensure that:
- Clinical detail is captured accurately
- The severity of illness is clearly represented
- Coding reflects the true scope of services
Beyond financial impact, better documentation also supports care coordination, quality reporting and clinical decision-making
Expanding Access Through Telehealth
Telehealth gives rural hospitals a way to expand access, connecting patients with specialists and offering more services without needing to invest in new physical infrastructure. This is especially important in areas like behavioral health, where provider shortages are common.
For rural hospitals, it offers a way to
- Connect patients with specialists who are not locally available
- Expand service offerings without significant infrastructure investment
- Reduce the need for patient travel
Leveraging Technology to Improve Efficiency and Visibility
Tools that help with documentation, automate routine workflows, and provide clearer data insights can reduce administrative burden and improve efficiency. And in rural healthcare, efficiency isn’t just about doing more with less, it can directly impact long-term stability.
Tools focused on documentation support, workflow automation, and data analytics
can help reduce administrative burden and improve overall efficiency.
For example:
- Automation can reduce manual tasks and speed up routine processes
- Analytics can provide visibility into performance trends, helping identify gaps and opportunities
- Decision-support tools can assist in improving accuracy and consistency
It’s Not Just About Staying Open, It’s About Staying Viable
One of the most important questions isn’t whether a rural hospital can stay open today, it’s whether it can continue operating in a sustainable way.
Running at a loss year after year isn’t a long-term solution.
Hospital leaders are often forced into difficult decisions:
Do we continue operating and risk financial collapse?
Do we scale back services to stay viable?
Do we transition to a different care model?
Or do we close entirely?
“Rural hospitals are navigating unprecedented financial and operational challenges that threaten their long-term viability.”
Martha Henley – CEO, Unity Medical Center
These aren’t just financial decisions. They directly affect access to care, community health, and the future of entire regions.
The Future of Rural Healthcare: Survival vs. Sustainability
For many rural hospitals, the conversation has already changed.
This isn’t about growth anymore, it’s about staying sustainable. The real challenge isn’t just improving performance metrics. It’s figuring out how to keep the doors open in an environment where financial pressure is constant, and, in many cases, intensifying.
Long-term sustainability will come down to how well hospitals adapt. And the landscape they’re adapting to isn’t easy: rising costs, tight reimbursements, workforce shortages, and changing patient expectations are all happening at once.
There’s no single playbook for this. What works in one community may not work in another. But a few patterns are starting to emerge.Some hospitals are reworking their operations to better match lower patient volumes, while still making sure essential services remain available.
Others are rethinking how care is delivered, blending in-person visits with outpatient and virtual care to create more flexible, accessible models. And many are focusing on getting their financial house in order, capturing revenue more effectively, reducing inefficiencies, and making every dollar count.
None of these changes are easy. But they’re becoming necessary.
The question isn’t just whether rural hospitals will survive.
It’s whether they can adapt fast enough to stay viable in a healthcare system that’s changing around them.
Because at the end of the day, this goes beyond hospitals. It’s about the people and communities who rely on them, often as their only source of care.
FAQs
1. Why are rural hospitals at risk of closure?
Rural hospitals face rising operating costs, lower reimbursement rates, and declining patient volumes. These financial pressures make it difficult to maintain sustainable operations over time.
2. What does it mean when a hospital has negative operating margins?
Negative margins mean the hospital is spending more money than it is earning from patient care. Sustained losses can quickly deplete reserves and threaten long-term viability.
3. What are the early warning signs of financial distress in rural hospitals?
Common signs include multi-year losses, rising denial rates, delayed payments, and reductions in services. These indicators often appear before closures occur.
4. Is accurate documentation important for hospital finances?
Incomplete records can lead to lower payments and lost revenue. It is important to have clear and complete documentation to ensure that the full complexity of care is reflected in reimbursement.
5. Is financial recovery possible for rural hospitals under pressure?
In many cases, yes. By strengthening processes, improving accuracy, and reducing inefficiencies, hospitals can stabilize finances even without major funding changes.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. I've led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let's connect to modernize workflows.