



















3 Payer Policy Changes Tightening E/M Billing Oversight in 2026
Evaluation and management (E/M) billing is entering a new phase of payer scrutiny. Across the healthcare industry, insurers are introducing stricter policies to monitor how providers document care, perform medical coding, and bill for E/M services. From modifier 25 reimbursement changes to automatic downcoding rules and peer-based coding comparisons, several payers are tightening oversight in an effort to control costs and improve billing accuracy.
For healthcare providers, these developments signal an important shift in reimbursement policy. As payers increase scrutiny of E/M claims, organizations must ensure their clinical documentation, medical coding practices, and compliance processes can withstand greater review.
Understanding these policy changes is essential for protecting revenue and maintaining compliance in an increasingly complex reimbursement environment
Why Are Payers Tightening Oversight on E/M Billing?
Several factors are driving increased scrutiny of evaluation and management billing across the healthcare industry.
Key reasons include:
- Rising healthcare costs and payer pressure to control spending
- Variation in E/M coding practices among providers
- Concerns about potential upcoding or inaccurate visit-level selection
- Updated E/M coding guidelines introduced in 2021
- The high volume of outpatient E/M claims submitted each year
Evaluation and management services represent one of the most common types of medical claims submitted to insurers. Industry estimates suggest that more than 40 percent of outpatient physician claims involve E/M services, making them one of the largest categories of professional reimbursement.
Because these services are submitted at such high volumes, even small changes in how payers review E/M claims can have significant financial implications for healthcare organizations.
At the same time, coding audits frequently reveal documentation gaps that affect the accuracy of E/M code selection. Healthcare revenue cycle studies have estimated that documentation deficiencies contribute to roughly 20–25 percent of medical claim denials, highlighting the close relationship between clinical documentation quality and reimbursement outcomes.
As a result, insurers are implementing new oversight mechanisms designed to ensure claims accurately reflect the complexity of care delivered.
How Documentation Quality Influences E/M Reimbursement?
Many of the challenges associated with E/M billing originate earlier in the clinical documentation and coding process. When documentation is incomplete or unclear, it increases the likelihood that payers will question the complexity level billed.
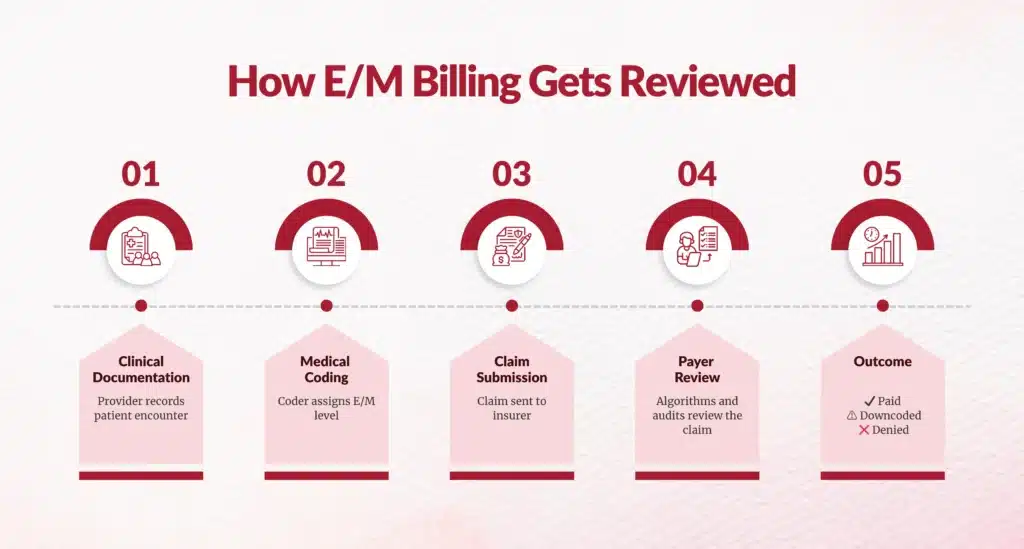
A simple framework illustrates how upstream documentation decisions influence downstream reimbursement outcomes.
Clinical Documentation
Providers record the patient encounter, including symptoms, diagnoses, medical decision-making, and treatment plans.
Coding Interpretation
Medical coders review the documentation and assign an evaluation and management code that reflects visit complexity.
Claim Submission
The claim is submitted to the payer with the selected E/M code and any applicable modifiers.
Payer Review
Insurers evaluate claims using automated claim edits, coding algorithms, and peer comparison analysis.
Financial Outcome
Claims may be reimbursed as billed, downcoded, delayed for review, or denied depending on documentation support.
This framework reinforces an important operational reality: documentation quality and coding discipline upstream often determine reimbursement stability downstream.
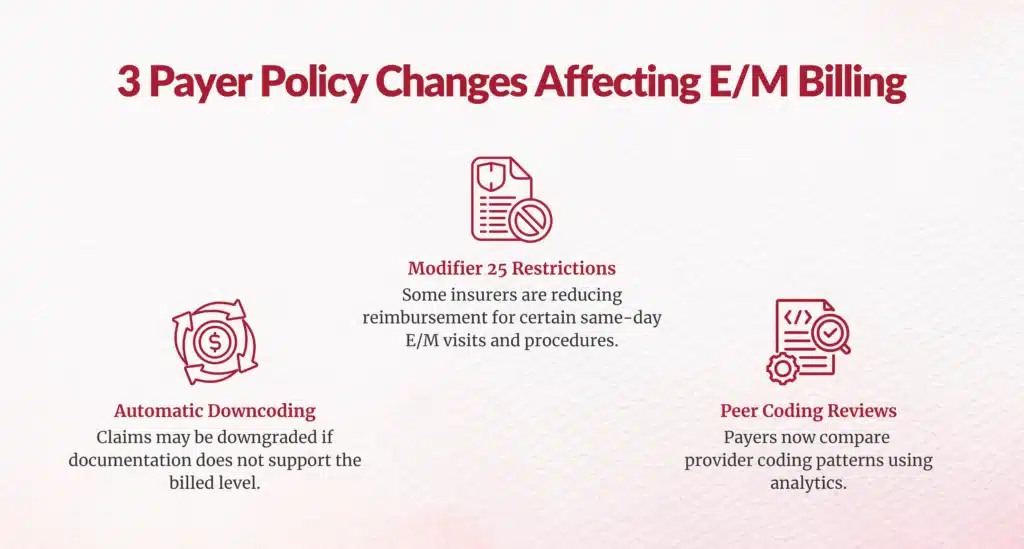
Recent Insurer Policies Increasing E/M Billing Scrutiny
Several major insurers have recently introduced policies designed to tighten oversight of evaluation and management coding.
These policies focus on modifier usage, coding complexity validation, and claim pattern analysis.
Below are three notable examples that illustrate how payer oversight is evolving.
How Modifier 25 Impacts E/M Reimbursement?
One of the most significant policy changes involves the use of modifier 25, which indicates that a significant and separately identifiable evaluation and management service was performed on the same day as another procedure.
Blue Cross Blue Shield of Michigan recently announced a policy that will reduce reimbursement by 50 percent for certain nonpreventive services billed with modifier 25. The policy primarily targets office visits that occur on the same day as a procedure.
The insurer’s reasoning is based on concerns that some evaluation services may duplicate work already included in the procedural reimbursement.
Many medical procedures include what is known as a global surgical period, which covers certain related services performed within a defined timeframe. These global periods can range from zero days to 90 days depending on the complexity of the procedure.
Initially, the policy included procedures with 90-day global periods. However, after provider feedback, the insurer revised the rule to exclude those procedures, limiting the reimbursement reduction to minor procedures with shorter global periods.
Certain scenarios will remain exempt from the policy. Emergency department visits occurring within one calendar day and nonsurgical procedures with no global period will not be affected.
Modifier 25 has historically been one of the most frequently reviewed modifiers in coding audits. Some industry assessments have found modifier-related documentation issues in approximately 15–20 percent of audited claims, making it a recurring source of reimbursement disputes.
Similar modifier 25 policies have faced resistance in the past. For example, Blue Cross Blue Shield of North Carolina withdrew a comparable policy shortly after announcing it in 2024 following provider concerns. Other insurers have delayed similar policies due to administrative and operational challenges.
How Automatic Downcoding Policies Work?
Another area receiving increased attention is the use of automatic downcoding policies.
Cigna introduced a policy that automatically downgrades certain outpatient E/M codes when documentation does not support the level of complexity billed.
Under this framework, claims submitted at higher complexity levels may be reduced to lower levels if the supporting documentation does not meet the payer’s internal review standards.
The insurer has indicated that the policy would affect only a small portion of claims. According to the payer, nearly 99 percent of in-network providers would not experience changes, and most providers billing higher complexity visits would remain unaffected.
However, provider organizations have raised several concerns.
One issue involves the appeals process. Early versions of the policy required providers to submit appeals through fax, which many healthcare groups view as outdated and inefficient.
Another concern involves potential conflicts with the E/M coding guideline changes introduced in 2021, which allow providers to determine E/M levels based on either medical decision-making complexity or the total time spent with the patient.
Providers often reference official resources such as the CY 2025 E/M Code List published by the Centers for Medicare & Medicaid Services for guidance. These guidelines allow providers to determine E/M levels based on either medical decision-making complexity or the total time spent managing the patient’s care.
Provider groups argue that payer-driven downcoding policies could create inconsistencies with nationally recognized coding standards.
How Peer Comparison Algorithms Flag Providers?
A third strategy insurers are adopting involves analyzing provider coding patterns using peer comparisons.
Under this model, insurers compare a provider’s E/M coding patterns with those of other clinicians who treat patients with similar risk profiles.
If a provider’s coding levels appear significantly different from peers, the insurer may initiate additional review before processing the claim.
Possible outcomes include:
- Requests for claim resubmission
- Temporary claim suspension
- Adjustments to reimbursement levels
This approach reflects a broader shift toward data-driven reimbursement oversight.
Rather than reviewing individual claims in isolation, payers are increasingly evaluating coding patterns across broader patient populations to identify potential billing anomalies.
Chirok Perspective: What These Policy Changes Mean for Providers
From Chirok’s perspective, the recent payer policies tightening E/M billing oversight represent a broader transformation in how insurers evaluate provider reimbursement behavior.
Historically, payer reviews focused primarily on individual claims. Today, insurers increasingly rely on analytics and large-scale claims datasets to evaluate coding patterns across providers, departments, and patient populations.
This shift means healthcare organizations are no longer being evaluated solely on isolated documentation decisions. Instead, payers are examining coding consistency and documentation integrity across entire provider groups.
As a result, several operational priorities are becoming increasingly important.
- The share of outpatient claims tied to E/M services
- The frequency of modifier 25 disputes in coding audits
- The percentage of denials tied to documentation gaps
The Share of Outpatient Claims Tied to E/M Services
Modifier-25 is one of the most frequently scrutinized coding modifiers in healthcare reimbursement audits. It is used to indicate that a significant, separately identifiable evaluation and management (E/M) service was performed on the same day as another procedure, allowing providers to bill for both services when documentation supports it.
However, because modifier-25 effectively “unbundles” services that would otherwise be packaged into a single payment, it has become a common trigger for payer reviews, denials, and coding audit disputes.
High Audit Scrutiny
Industry analyses consistently show that modifier-25 is among the most audited modifiers in healthcare claims, alongside modifier-59. Coding audits frequently focus on whether the E/M service documented truly qualifies as “significant and separately identifiable” from the procedure performed.
Government agencies and commercial payers track the use of modifier-25 closely because patterns of overuse may indicate improper billing or documentation gaps.
Improper Use Identified in Federal Audits
Federal reviews have highlighted how often modifier-25 claims fail documentation standards. For example:
- A U.S. Office of Inspector General (OIG) analysis found that approximately 35% of Medicare claims containing modifier-25 did not meet program requirements.
- In another federal audit examining ophthalmology injections, documentation supporting modifier-25 was insufficient in 22 out of 24 sampled claims, indicating a very high rate of non-compliance in the reviewed cases.
These findings explain why payers frequently challenge modifier-25 usage during coding audits.
Why Modifier-25 Triggers Frequent Disputes?
Several factors contribute to the high rate of disputes involving modifier-25:
- Documentation ambiguity – Providers may document routine pre-procedure evaluation rather than a distinct E/M service.
- Overuse in certain specialties – Specialties with frequent minor procedures (dermatology, ophthalmology, orthopedics) tend to apply modifier-25 more often.
- Payer interpretation differences – Coders may consider a service separately identifiable, while payers may consider it bundled into the procedure.
- Automated payer algorithms – Many insurers use analytics to flag claims with modifier-25 for manual review.
Impact on Coding Audits
Because of these risks, modifier-25 usage is routinely evaluated in internal and external audits. Auditors typically examine:
- E/M documentation depth and medical decision-making
- Clinical necessity separate from the procedure
- Consistency in modifier usage patterns across providers
- Specialty-specific benchmarks and peer comparison
As a result, modifier-25 disputes remain one of the most common issues identified during medical coding audits, often leading to claim denials, payment recoupments, or compliance investigations if documentation cannot justify the modifier.
The Percentage of Denials Tied to Documentation Gaps
Documentation gaps remain one of the leading causes of claim denials across the healthcare revenue cycle. Industry research indicates that nearly 50–65% of claim denials are linked to missing, incomplete, or inaccurate documentation in the patient record.
Documentation issues can occur at multiple points in the care and billing workflow, including:
- Insufficient clinical detail to support the billed CPT or HCPCS code
- Missing physician signatures or authentication
- Incomplete medical necessity documentation
- Lack of supporting notes for procedures or E/M levels
- Missing prior authorization documentation
Because payer reimbursement decisions depend heavily on clinical documentation, even minor gaps can trigger denials or requests for additional information.
Documentation Gaps and Revenue Cycle Risk
Studies from revenue cycle management organizations and healthcare financial groups have shown that documentation deficiencies account for a significant portion of medical necessity denials and coding disputes. These issues are especially common in high-volume outpatient services such as:
- Evaluation and Management (E/M) visits
- Diagnostic imaging
- Surgical procedures requiring prior authorization
- Specialty services with complex coding requirements
When documentation does not clearly support the billed service, payers often deny the claim outright or require time-consuming appeals. As a result, healthcare organizations increasingly prioritize clinical documentation improvement (CDI) programs and coding audits to reduce denial rates.
Why This Matters for Coding Audits?
Because documentation gaps drive a large share of denials, coding audits frequently focus on:
- Documentation completeness
- Alignment between clinical notes and CPT/ICD-10 codes
- Medical necessity support
- Modifier justification (such as modifier-25 or modifier-59)
Strengthening documentation practices can significantly reduce preventable denials and improve reimbursement accuracy.
The Share of Outpatient Claims Tied to E/M Services
Evaluation and Management (E/M) services represent one of the largest categories of outpatient medical claims. Studies analyzing national claims data have found that E/M services account for roughly 35% of outpatient medical claims, making them the single largest service category in ambulatory care.
These services include patient encounters such as:
- Office visits with primary care physicians
- Specialist consultations
- Emergency department evaluation visits
- Telehealth consultations
- Behavioral health assessments
Because E/M services are tied to routine patient evaluation and care coordination rather than procedures, they occur frequently across outpatient settings. As a result, a significant share of healthcare interactions, especially primary care and chronic disease management, are billed under E/M CPT codes.
In addition to their high claim volume, E/M services also account for a substantial portion of healthcare spending. In some insurance populations, payments for E/M services represent more than 40% of spending on certain outpatient service categories, highlighting their central role in reimbursement and revenue cycle operations.
Why This Matters for Coding and Audits?
Because E/M claims make up such a large share of outpatient activity, they are also a major focus of coding compliance efforts. Documentation accuracy, coding level selection, and modifier usage, such as modifier-25, are frequently audited to ensure that services are properly supported in the medical record.
How Modifier 25 Impacts E/M Reimbursement?
Modifier 25 allows providers to report a significant and separately identifiable evaluation and management service on the same day as another procedure. Because this modifier directly influences how E/M services are reimbursed alongside procedures, payers often review these claims closely to confirm that documentation clearly supports the additional evaluation work performed.
How Automatic Downcoding Policies Work?
Automatic downcoding policies allow insurers to review submitted E/M codes and reduce the complexity level if the documentation does not support the billed service. These policies have become an increasingly discussed issue within the healthcare revenue cycle community and are frequently highlighted at MGMA conferences.
How Peer Comparison Algorithms Flag Providers?
Many insurers now use peer comparison models to analyze coding patterns. Under this approach, a provider’s E/M coding distribution is compared with clinicians treating similar patient populations. When coding patterns differ significantly from peer benchmarks, the payer may initiate additional review or request further documentation.
Organizations that invest in documentation quality, coding analytics, and proactive compliance monitoring are better positioned to navigate an environment where payer scrutiny continues to intensify.
Key Takeaways
- Insurers are increasing oversight of evaluation and management billing.
- Modifier 25 policies are receiving increased scrutiny.
- Automatic downcoding policies are expanding across insurers.
- Peer comparison models allow payers to analyze coding patterns across providers.
- Documentation quality and coding consistency play a major role in reimbursement stability.
Preparing for Greater Payer Scrutiny
As payer oversight increases, healthcare organizations should take proactive steps to strengthen coding compliance.
Operational strategies may include:
Monitor modifier 25 utilization by specialty
Certain specialties rely more heavily on same-day procedures and office visits. Tracking modifier 25 usage patterns by specialty can help identify unusual billing trends.
Conduct targeted coding audits
Regular audits of high-volume E/M services can help identify documentation gaps before they trigger payer review.
Track E/M complexity patterns across clinicians
Analytics tools can reveal variations in coding levels among providers treating similar patient populations.
Review payer-specific downcoding trends
Monitoring reimbursement patterns across insurers can help organizations detect emerging policy changes earlier.
Assessing Your E/M Billing Risk
As payer oversight continues to expand, healthcare organizations may benefit from conducting a focused review of their E/M billing practices.
A targeted E/M risk assessment often includes reviewing:
- Documentation support for E/M complexity levels
- Modifier 25 utilization patterns
- Coding variation across clinicians
- Denial or downcoding trends
- Payer-specific reimbursement policy changes
Identifying potential coding vulnerabilities early can help organizations reduce reimbursement disruptions and maintain revenue stability.




Final Thoughts
The recent policies introduced by multiple insurers suggest that tighter oversight of evaluation and management billing will likely continue.
As healthcare costs rise and payers seek greater reimbursement transparency, E/M services will remain a key focus of billing compliance efforts.
Healthcare organizations that prioritize documentation accuracy, medical coding integrity, and proactive compliance strategies will be better prepared to navigate this evolving reimbursement landscape.
FAQs
1. What is E/M billing?
Evaluation and management billing refers to medical codes used to report patient visits and clinical encounters. These codes reflect the complexity of care provided, including medical decision-making and the time spent managing a patient’s condition.
2. What is modifier 25?
Modifier 25 indicates that a significant and separately identifiable evaluation and management service was provided on the same day as another procedure.
3. What is downcoding?
Downcoding occurs when a payer reduces the complexity level of a billed service because the submitted documentation does not support the higher-level code.
4. Why are insurers increasing scrutiny of E/M coding?
Insurers are increasing oversight to control healthcare spending, reduce improper payments, and ensure billing accuracy.
Author Bio:

Kanar Kokoy
CEO - Chirok Health
Healthcare CEO & CDI/RCM innovator. I help orgs boost accuracy, integrity & revenue via truthful clinical docs. Led transformations in CDI, coding, AI solutions, audits & VBC for health systems, ACOs & more. Let’s connect to modernize workflows.